
Hansen can be filled out without any problem. Simply try FormsPal PDF editor to do the job quickly. To make our tool better and less complicated to work with, we consistently design new features, taking into consideration suggestions coming from our users. Starting is simple! All that you should do is take the following simple steps down below:
Step 1: First of all, open the pdf tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: With our advanced PDF tool, you're able to accomplish more than just complete blank form fields. Edit away and make your docs look perfect with customized textual content put in, or fine-tune the original input to perfection - all that comes along with an ability to incorporate stunning pictures and sign it off.
As for the blanks of this particular form, this is what you should know:
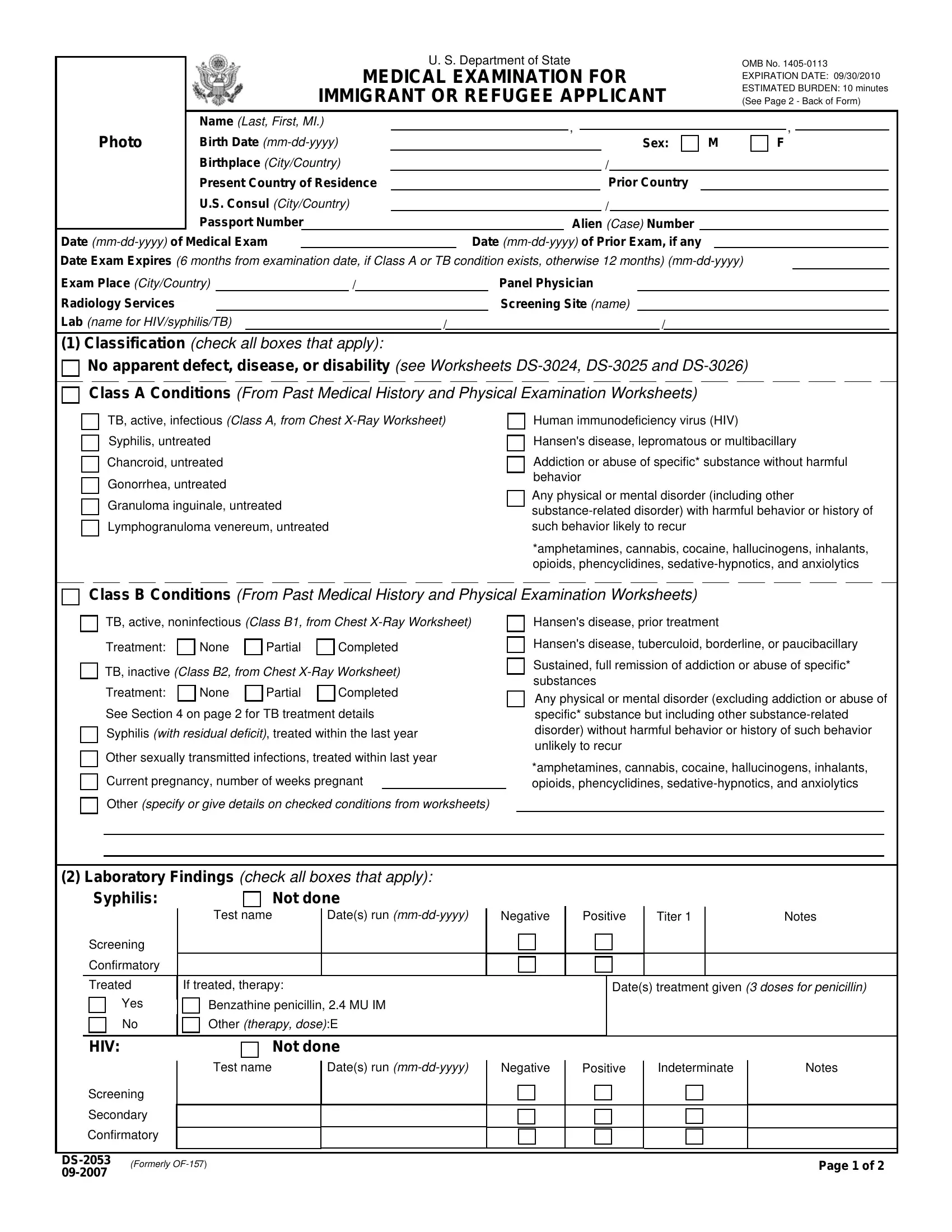
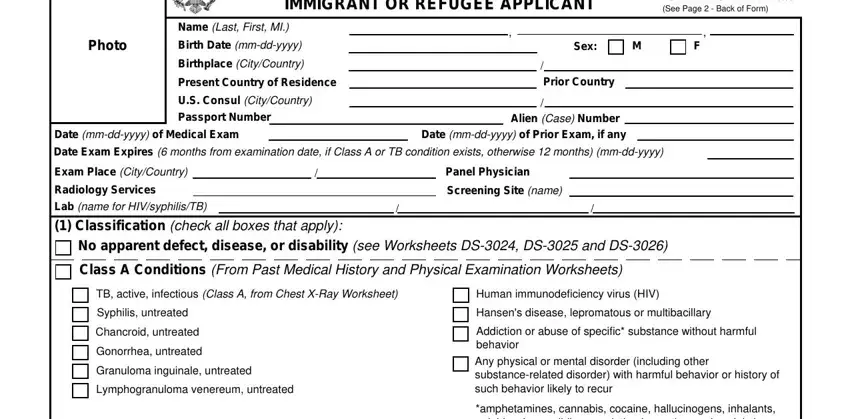
1. The Hansen involves specific details to be typed in. Make certain the subsequent fields are complete:
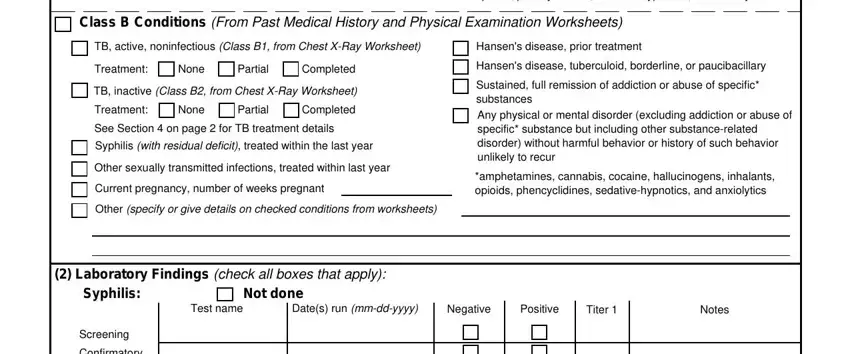
2. The third stage is to submit all of the following fields: amphetamines cannabis cocaine, Class B Conditions From Past, TB active noninfectious Class B, Hansens disease prior treatment, Treatment, None, Partial, Completed, TB inactive Class B from Chest, Treatment, None, Partial, Completed, See Section on page for TB, and Syphilis with residual deficit.
3. This next step will be about Confirmatory, Treated, If treated therapy, Dates treatment given doses for, Benzathine penicillin MU IM, Other therapy doseE Not done, Test name, Dates run mmddyyyy, Negative, Positive, Indeterminate, Notes, Yes, HIV, and Screening - fill in each one of these empty form fields.
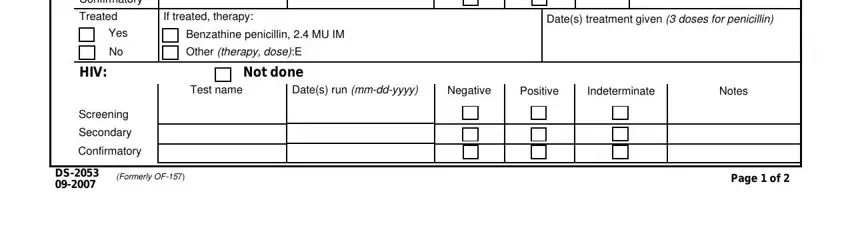
It is easy to get it wrong while filling in the Notes, for that reason make sure to reread it prior to when you submit it.
4. To move onward, this next part involves completing a couple of empty form fields. Examples include Immunizations See Vaccination, Vaccine history complete, Vaccine history incomplete, Incomplete vaccine history no, Blanket waiver, Individual waiver, I certify that I understand the, Applicant Signature, Panel Physician Signature, Date mmddyyyy, Tuberculosis Treatment Regimen, Fill out if applicant has taken in, Check if therapy currently, Medication, and DoseInterval ie mgday, which are vital to going forward with this process.
5. The form should be wrapped up by dealing with this section. Here you'll see a detailed list of blank fields that need to be filled out with correct information for your form submission to be accomplished: Pyrazinamide, Ethambutol, Streptomycin, Other specify, Applicants weight kg, and Remarks.
Step 3: Check that your information is accurate and click on "Done" to complete the task. Download the Hansen the instant you subscribe to a 7-day free trial. Readily view the pdf document inside your FormsPal account, together with any modifications and changes all saved! FormsPal is invested in the confidentiality of our users; we make sure all personal data going through our tool is kept confidential.