The form e3065 filling out course of action is quick. Our software lets you work with any PDF file.
Step 1: Get the button "Get Form Here" and select it.
Step 2: You are now able to modify form e3065. You possess plenty of options with our multifunctional toolbar - you can include, erase, or change the content material, highlight the particular components, and perform several other commands.
The next areas are included in the PDF form you'll be creating.
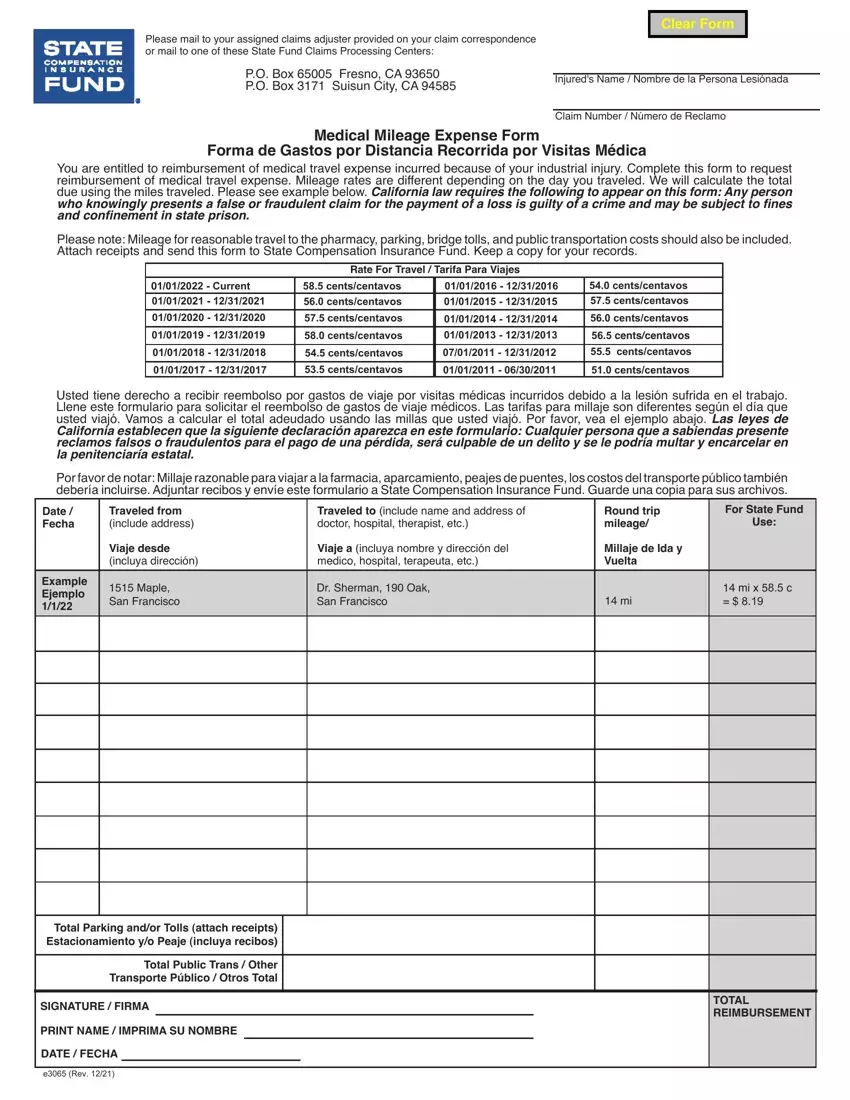
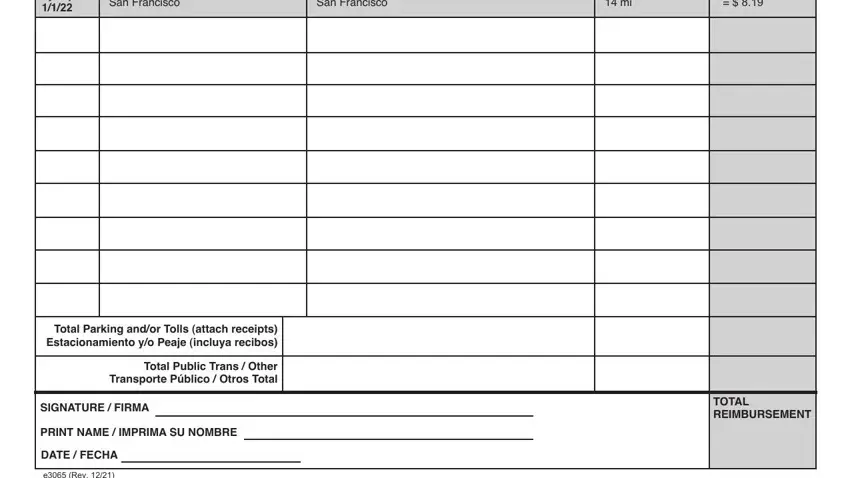
Provide the necessary data in the Example Ejemplo, Maple San Francisco, Dr Sherman Oak San Francisco, mi x c, Total Parking andor Tolls attach, Total Public Trans Other, SIGNATURE FIRMA, PRINT NAME IMPRIMA SU NOMBRE, DATE FECHA, e Rev, and TOTAL REIMBURSEMENT area.
Step 3: Choose the Done button to save your form. At this point it is obtainable for export to your device.
Step 4: To prevent different hassles in the foreseeable future, be sure to generate up to two or three duplicates of the file.
