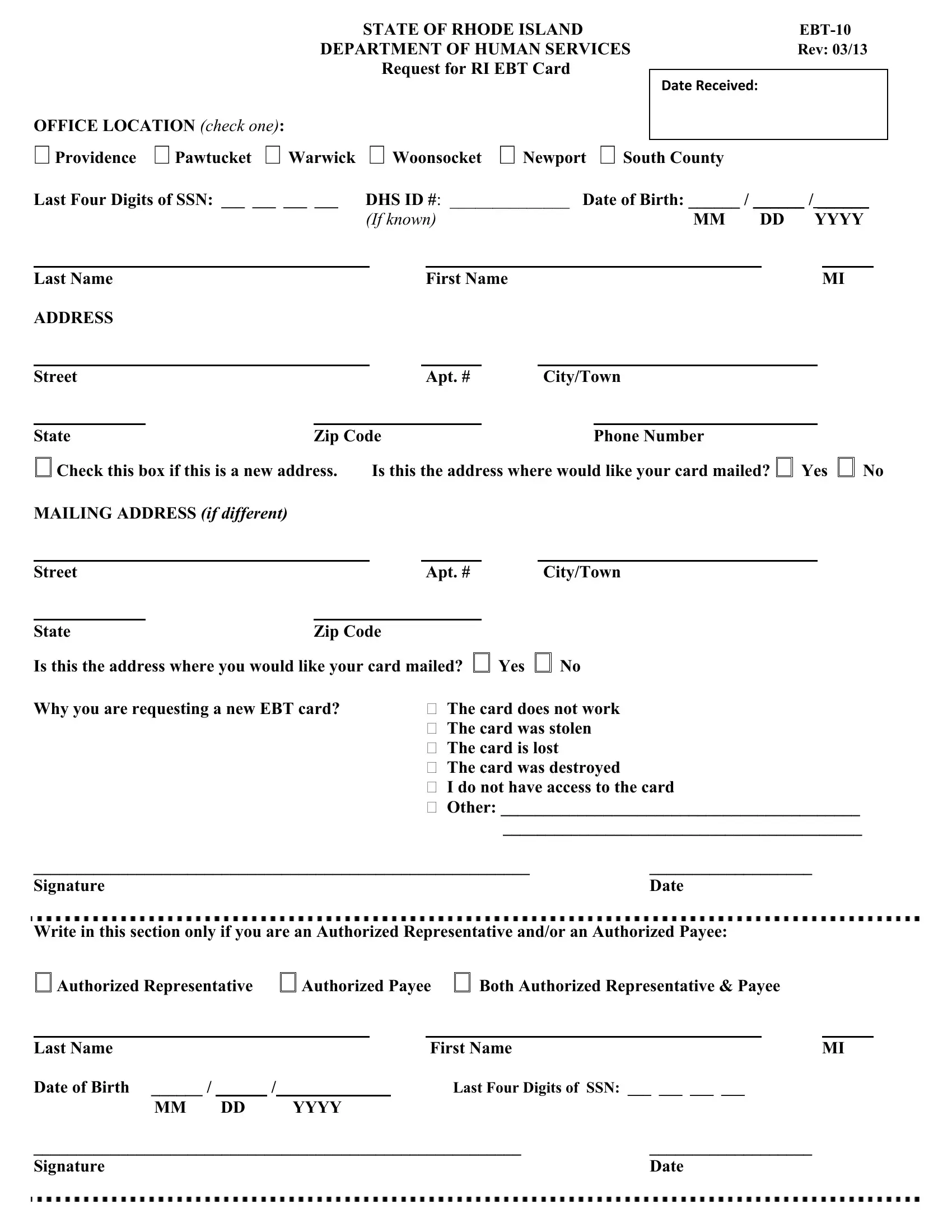
In the realm of public assistance in the State of Rhode Island, the Electronic Benefit Transfer (EBT) system plays a pivotal role, facilitating the seamless distribution of benefits to individuals in need. Among the documents integral to this system is the EBT-10 form, designed by the Rhode Island Department of Human Services. Revised last in March 2013, this form serves as a request for a new Rhode Island EBT Card, a crucial tool for accessing benefits such as food assistance and cash benefits. The form is comprehensive, requesting information including, but not limited to, the last four digits of the Social Security number, Department of Human Services (DHS) ID number, as well as personal identification details like name, date of birth, and contact information. Importantly, it asks the applicant to specify the reason for the new card request—options include malfunction, theft, loss, destruction of the previous card, lack of access, or other reasons necessitating a replacement. Additionally, it caters to individuals acting as authorized representatives or payees, incorporating sections for their information and signatures. This document embodies a critical step for recipients in maintaining uninterrupted access to their entitled benefits, underlining the broader commitment to supporting those facing hardships within the state.
| Question | Answer |
|---|---|
| Form Name | Form Ebt 10 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ebt ri form |
|
|
|
STATE OF RHODE ISLAND |
|
|
|
|
|||||||||
|
|
DEPARTMENT OF HUMAN SERVICES |
Rev: 03/13 |
|
||||||||||||
|
|
|
|
Request for RI EBT Card |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
DATE RECEIVED: |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
OFFICE LOCATION (CHECK ONE): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Providence |
Pawtucket Warwick |
Woonsocket |
Newport |
|
|
|
|
|
|
|||||||
South County |
|
|
|
|
||||||||||||
Last Four Digits of SSN: ___ ___ ___ ___ |
DHS ID #: ______________ Date of Birth: ______ / ______ / ______ |
|
||||||||||||||
|
|
|
(IF KNOWN) |
|
|
|
MM DD |
YYYY |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name |
|
|
|
|
|
First Name |
|
|
|
|
|
MI |
|
|||
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street |
|
|
|
|
|
Apt. # |
|
City/Town |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
State |
|
Zip Code |
|
|
Phone Number |
|
|
|
|
|||||||
Check this box if this is a new address.
MAILING ADDRESS (IF DIFFERENT)
Street
Is this the address where would like your card mailed? Yes No
Apt. # |
City/Town |
State |
Zip Code |
|
|
|
Is this the address where you would like your card mailed? |
Yes |
No |
||
Why you are requesting a new EBT card? |
The card does not work |
|||
The card was stolen
The card is lost
The card was destroyed
I do not have access to the card
Other: __________________________________________
__________________________________________
__________________________________________________________ |
___________________ |
Signature |
Date |
Write in this section only if you are an Authorized Representative and/or an Authorized Payee:
Authorized Representative |
Authorized Payee |
Both Authorized Representative & Payee |
||||||||
|
|
|
|
|
|
|
|
|
|
|
Last Name |
|
|
|
|
|
First Name |
|
|
MI |
|
Date of Birth ______ / ______ / |
_________ |
|
|
Last Four Digits of SSN: ___ ___ ___ ___ |
||||||
MM |
DD |
|
YYYY |
|
|
|
|
|
||
_________________________________________________________ |
___________________ |
|
||||||||
Signature |
|
|
|
|
|
|
|
Date |
||