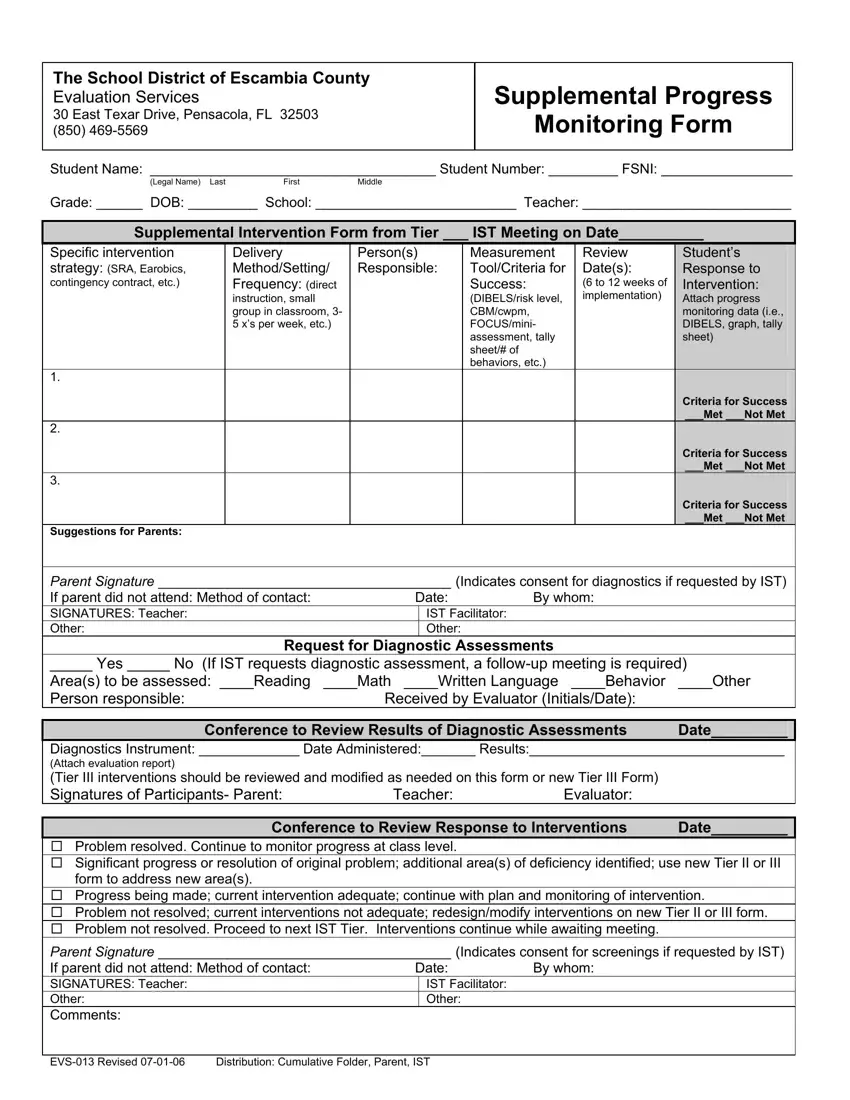
In the heart of Escambia County, Florida, the School District's Evaluation Services team has crafted a vital document for assisting students who need extra academic or behavioral support: the EVS 013 form, otherwise known as the Supplemental Progress Monitoring Form. Positioned at 30 East Texar Drive in Pensacola, this team stands ready to use this form as a cornerstone for evaluating and enhancing student progress through tailored interventions. Designed to closely monitor the effectiveness of specific strategies implemented to improve a student's performance, this form spans from delineating student information, such as name, grade, and school, to recording intricate details of interventions, including the type, frequency, and personnel involved. Special sections are devoted to assessing the intervention's success over 6 to 12 weeks, offering a clear criteria-based evaluation and next steps, whether that be continuing, adjusting, or escalating the interventions. Furthermore, the form extends its utility by soliciting parent involvement through consent for diagnostic assessments or screenings and capturing their signatures, thereby ensuring a collaborative effort between teachers, evaluators, and families. This form is not just paperwork; it's a pivotal tool in making informed decisions that directly impact the student's educational journey, embodying a structured approach to tailor and refine educational support where it's needed most.
| Question | Answer |
|---|---|
| Form Name | Form Evs 013 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Earobics, SRA, progress monitoring forms pdf, Escambia |
The School District of Escambia County
Evaluation Services
30 East Texar Drive, Pensacola, FL 32503
(850)
Supplemental Progress
Monitoring Form
Student Name: _____________________________________ Student Number: _________ FSNI: _________________
(Legal Name) LastFirstMiddle
Grade: ______ DOB: _________ School: __________________________ Teacher: ___________________________
Supplemental Intervention Form from Tier ___ IST Meeting on Date__________
Specific intervention |
Delivery |
Person(s) |
Measurement |
Review |
|
Student’s |
|
strategy: (SRA, Earobics, |
Method/Setting/ |
Responsible: |
Tool/Criteria for |
Date(s): |
|
Response to |
|
contingency contract, etc.) |
Frequency: (direct |
|
Success: |
(6 to 12 weeks of |
|
Intervention: |
|
|
instruction, small |
|
(DIBELS/risk level, |
implementation) |
|
Attach progress |
|
|
|
|
|
|
|||
|
group in classroom, 3- |
|
CBM/cwpm, |
|
|
monitoring data (i.e., |
|
|
5 x’s per week, etc.) |
|
FOCUS/mini- |
|
|
DIBELS, graph, tally |
|
|
|
|
assessment, tally |
|
|
sheet) |
|
|
|
|
sheet/# of |
|
|
|
|
|
|
|
behaviors, etc.) |
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Criteria for Success |
|
|
|
|
|
|
|
___Met ___Not Met |
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Criteria for Success |
|
|
|
|
|
|
|
___Met ___Not Met |
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Criteria for Success |
|
|
|
|
|
|
|
___Met ___Not Met |
|
Suggestions for Parents: |
|
|
|
|
|
|
|
Parent Signature ______________________________________ (Indicates consent for diagnostics if requested by IST)
If parent did not attend: Method of contact: |
Date: |
By whom: |
|
|
SIGNATURES: Teacher: |
|
IST Facilitator: |
|
|
Other: |
|
Other: |
|
|
Request for Diagnostic Assessments |
|
|||
_____ Yes _____ No (If IST requests diagnostic assessment, a |
||||
Area(s) to be assessed: ____Reading |
____Math ____Written Language ____Behavior |
____Other |
||
Person responsible: |
Received by Evaluator (Initials/Date): |
|
||
|
|
|||
Conference to Review Results of Diagnostic Assessments |
Date_________ |
|||
Diagnostics Instrument: _____________ Date Administered:_______ Results:_________________________________
(Attach evaluation report)
(Tier III interventions should be reviewed and modified as needed on this form or new Tier III Form)
Signatures of Participants- Parent: |
Teacher: |
Evaluator: |
|
|
|
||
Conference to Review Response to Interventions |
Date_________ |
||
Problem resolved. Continue to monitor progress at class level.
Significant progress or resolution of original problem; additional area(s) of deficiency identified; use new Tier II or III form to address new area(s).
Progress being made; current intervention adequate; continue with plan and monitoring of intervention.
Problem not resolved; current interventions not adequate; redesign/modify interventions on new Tier II or III form.
Problem not resolved. Proceed to next IST Tier. Interventions continue while awaiting meeting.
Parent Signature ______________________________________ (Indicates consent for screenings if requested by IST)
If parent did not attend: Method of contact: |
Date: |
By whom: |
||
SIGNATURES: Teacher: |
|
|
IST Facilitator: |
|
Other: |
|
|
Other: |
|
Comments: |
|
|
|
|
|
|
|
||
Distribution: Cumulative Folder, Parent, IST |
|
|||
