
It is possible to fill in prior authorization wisconsin online instantly using our PDFinity® online tool. Our tool is constantly evolving to grant the very best user experience attainable, and that is thanks to our commitment to continuous enhancement and listening closely to customer feedback. Starting is simple! Everything you need to do is follow the following simple steps directly below:
Step 1: Click the orange "Get Form" button above. It is going to open our editor so that you can begin filling out your form.
Step 2: With our online PDF editor, you can do more than just fill in forms. Edit away and make your docs seem faultless with customized text added, or fine-tune the file's original content to perfection - all comes with the capability to add stunning graphics and sign the document off.
This PDF form requires some specific information; in order to ensure accuracy and reliability, make sure you bear in mind the tips just below:
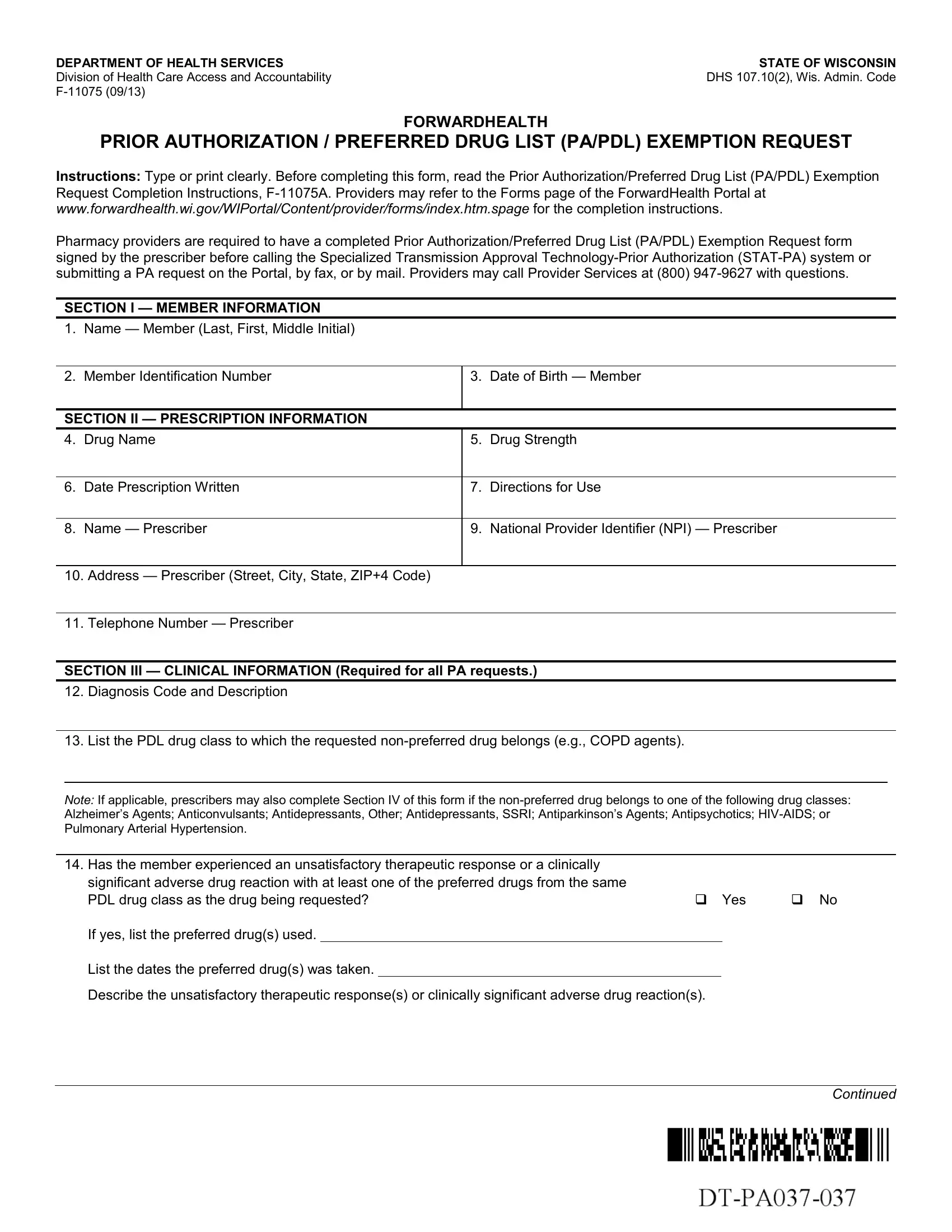
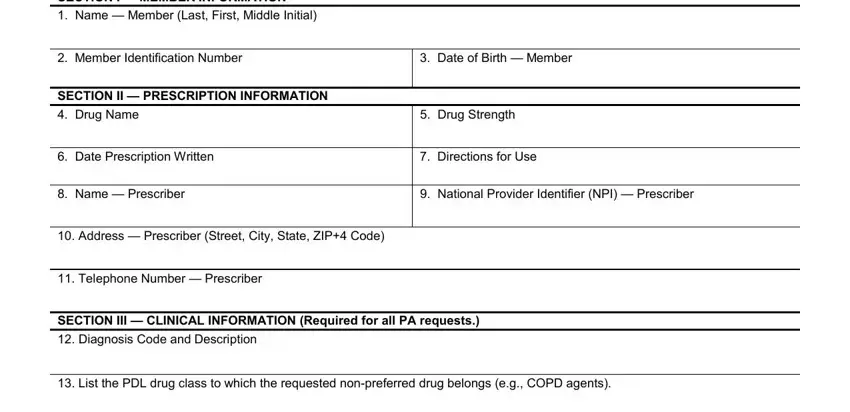
1. The prior authorization wisconsin online usually requires certain details to be typed in. Ensure the next fields are finalized:
2. Once the previous part is complete, it's time to include the required specifics in Has the member experienced an, significant adverse drug reaction, Yes, If yes list the preferred drugs, List the dates the preferred drugs, Describe the unsatisfactory, and Continued so that you can move on further.
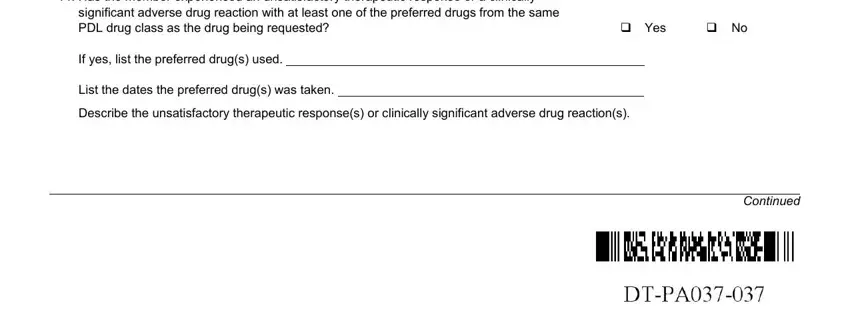
Be really mindful when completing Has the member experienced an and Yes, as this is where a lot of people make mistakes.
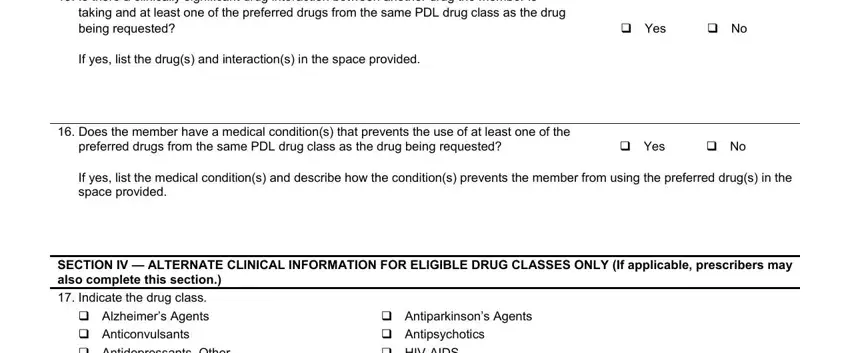
3. This next stage will be hassle-free - complete all the fields in Is there a clinically significant, taking and at least one of the, If yes list the drugs and, Yes, Does the member have a medical, preferred drugs from the same PDL, Yes, If yes list the medical conditions, SECTION IV ALTERNATE CLINICAL, Indicate the drug class, and Antiparkinsons Agents in order to complete this part.
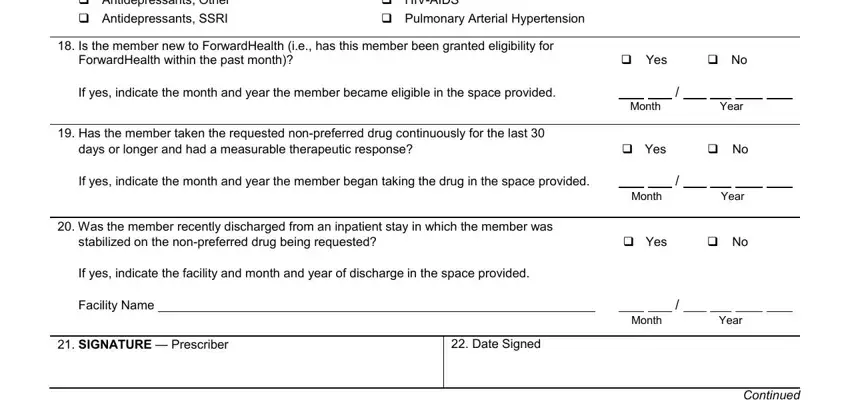
4. The form's fourth subsection comes next with the next few blanks to fill out: Indicate the drug class, Antiparkinsons Agents, Is the member new to, ForwardHealth within the past month, Yes, If yes indicate the month and year, Month, Year, Has the member taken the, days or longer and had a, Yes, If yes indicate the month and year, Month, Year, and Was the member recently.
5. As you approach the end of this form, there are actually a few extra requirements that have to be met. Mainly, SECTION V FOR PHARMACY PROVIDERS, National Drug Code Digits, Days Supply Requested Up to Days, NPI, Date of Service MMDDCCYY For, days in the past, Place of Service, Assigned PA Number, Grant Date, Expiration Date, Number of Days Approved, SECTION VI ADDITIONAL INFORMATION, Include any additional, and drug requested may be included here must all be filled out.
Step 3: Reread what you have inserted in the form fields and click the "Done" button. Obtain the prior authorization wisconsin online the instant you sign up at FormsPal for a free trial. Easily gain access to the document within your FormsPal account page, together with any edits and changes all synced! Here at FormsPal, we aim to be sure that your details are maintained protected.