FB-0187-0612w
STATE OF NEW JERSEY – DEPARTMENT OF THE TREASURY
DIVISION OF PENSIONS AND BENEFITS
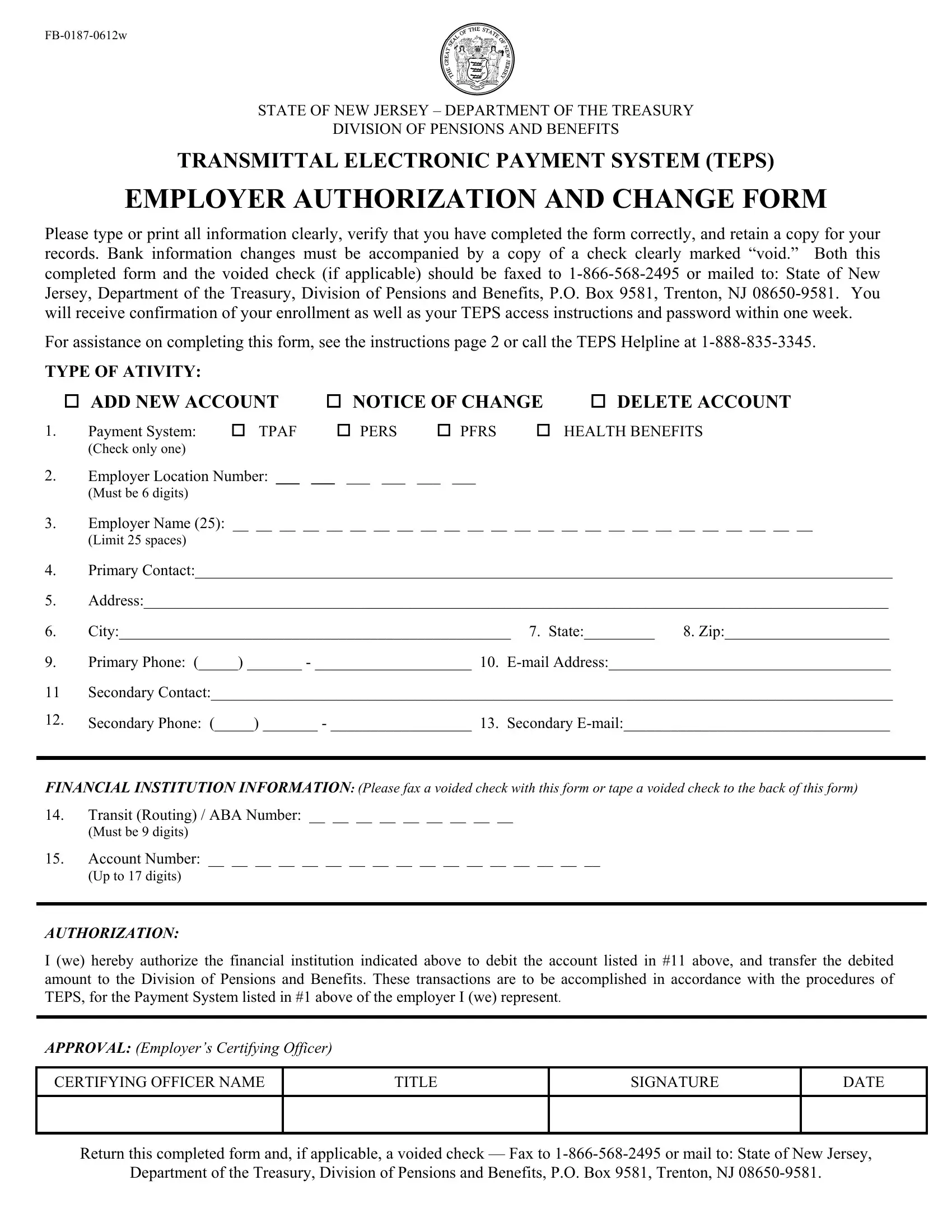
TRANSMITTAL ELECTRONIC PAYMENT SYSTEM (TEPS)
EMPLOYER AUTHORIZATION AND CHANGE FORM
Please type or print all information clearly, verify that you have completed the form correctly, and retain a copy for your records. Bank information changes must be accompanied by a copy of a check clearly marked “void.” Both this completed form and the voided check (if applicable) should be faxed to 1-866-568-2495 or mailed to: State of New Jersey, Department of the Treasury, Division of Pensions and Benefits, P.O. Box 9581, Trenton, NJ 08650-9581. You will receive confirmation of your enrollment as well as your TEPS access instructions and password within one week.
For assistance on completing this form, see the instructions page 2 or call the TEPS Helpline at 1-888-835-3345.
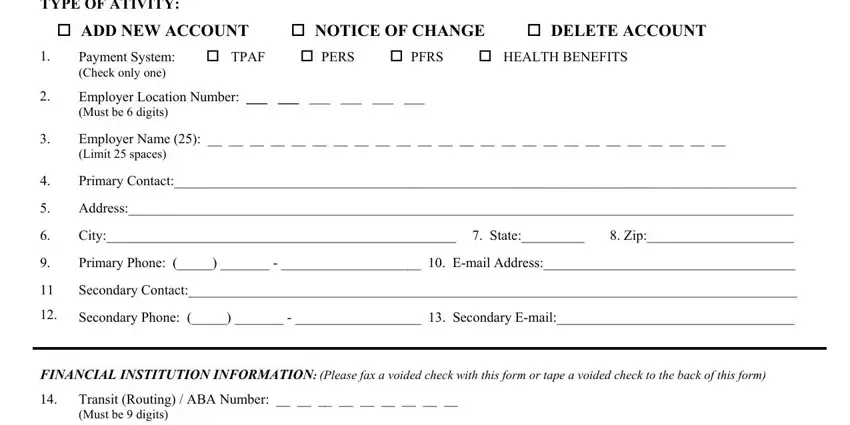
TYPE OF ATIVITY:
ADD NEW ACCOUNT |
NOTICE OF CHANGE |
DELETE ACCOUNT |
1. Payment System: |
TPAF |
PERS |
PFRS |
HEALTH BENEFITS |
(Check only one) |
|
|
|
|
2.Employer Location Number: ___ ___ ___ ___ ___ ___
(Must be 6 digits)
3. Employer Name (25): __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
(Limit 25 spaces)
4.Primary Contact:_________________________________________________________________________________________
5.Address:_______________________________________________________________________________________________
6. |
City:__________________________________________________ 7. State:_________ |
8. Zip:_____________________ |
9.Primary Phone: (_____) _______ - ____________________ 10. E-mail Address:____________________________________
11Secondary Contact:_______________________________________________________________________________________
12.Secondary Phone: (_____) _______ - __________________ 13. Secondary E-mail:__________________________________
FINANCIAL INSTITUTION INFORMATION: (Please fax a voided check with this form or tape a voided check to the back of this form)
14.Transit (Routing) / ABA Number: __ __ __ __ __ __ __ __ __
(Must be 9 digits)
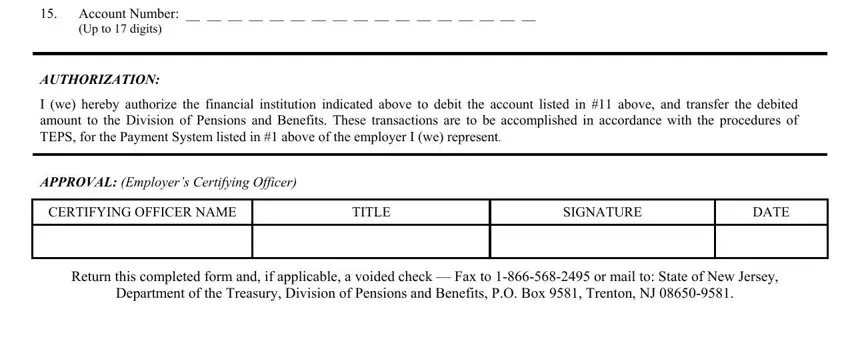
15. Account Number: __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
(Up to 17 digits)
AUTHORIZATION:
I (we) hereby authorize the financial institution indicated above to debit the account listed in #11 above, and transfer the debited amount to the Division of Pensions and Benefits. These transactions are to be accomplished in accordance with the procedures of TEPS, for the Payment System listed in #1 above of the employer I (we) represent.
APPROVAL: (Employer’s Certifying Officer)
Return this completed form and, if applicable, a voided check — Fax to 1-866-568-2495 or mail to: State of New Jersey,
Department of the Treasury, Division of Pensions and Benefits, P.O. Box 9581, Trenton, NJ 08650-9581.
FB-0187-0612w
STATE OF NEW JERSEY – DEPARTMENT OF THE TREASURY
DIVISION OF PENSIONS AND BENEFITS
TRANSMITTAL ELECTRONIC PAYMENT SYSTEM (TEPS)
EMPLOYER AUTHORIZATION AND CHANGE FORM
INSTRUCTIONS
This form is to be used for first-time enrollment in TEPS and also to make changes to your TEPS enrollment information.
ADD NEW ACCOUNT: For employers registering for a new payment system in the TEPS program.
NOTICE OF CHANGE: Used by employers to change the TEPS information on file, e.g., new address, different financial institution ABA and/or account, additional retirement ACH account combination, etc.
DELETE ACCOUNT: Submitted to terminate TEPS participation for a particular retirement system.
You must complete ALL items on the form. Omitted or illegible information in any section will automatically prohibit processing and guarantee the immediate return of your form for proper completion.
1. |
PAYMENT SYSTEM: |
Check the appropriate payment system. A separate Authorization Form must be completed |
|
|
|
for each payment system and location number. |
2. |
EMPLOYER LOCATION |
Your 6-digit Location Number. TPAF accounts with 3 or 4 digits must include leading |
|
NUMBER: |
|
zeros (i.e. 100xxx or 10xxxx). |
3. |
EMPLOYER NAME: |
Please use the spaces (up to 25 characters) to print/type the name exactly as it should |
|
|
|
appear for presentation of the ACH item to the financial institutions. |
4. |
PRIMARY CONTACT: |
Name of the individual designated as the primary TEPS contact, who can be contacted in |
|
|
|
the event of questions concerning this form or future payments. |
5. |
ADDRESS: |
6. CITY: |
Please indicate the correct mailing address for proper delivery of all TEPS correspondence. |
7. |
STATE: |
8. ZIP CODE: |
Please include the two-digit state abbreviation and your 5-digit zip or 9-digit (zip+4) code. |
9.PRIMARY CONTACT PHONE: The direct telephone number of the primary contact named in item # 4.
10.PRIMARY CONTACT E-MAIL: The e-mail address of the primary contact named in item # 4.
11.SECONDARY CONTACT: Name of the individual designated as the secondary TEPS contact, who can be contacted in the event of questions concerning this form or future payments.
12.SECONDARY CONTACT PHONE: List the direct telephone number of the secondary contact.
13. |
SECONDARY CONTACT |
List the e-mail address of the secondary contact. |
|
E-MAIL: |
|
14. |
FINANCIAL INSTITUTION |
The 9-digit ABA/Transit Routing Number used to identify the financial institution at which |
|
TRANSIT/ABA NUMBER: |
the employer maintains their account. This number appears in the bottom line of the |
|
|
checks. |
15. |
ACCOUNT NUMBER: |
The account identification number used to fund your transmittal (up to 17 digits). This |
|
|
must be a checking account. |
AUTHORIZATION AND APPROVAL |
The Certifying Officer must sign and date this area. |
OF CERTIFYING OFFICER: |
|
|
|
|
|
|
|
Please fax the completed form to: 1-866-568-2495 or mail to: State of New Jersey, Department of the Treasury, Division of Pensions and Benefits, P.O. Box 9581, Trenton, NJ 08650-9581. You will receive confirmation of your enrollment as well as your TEPS access instructions and password within one week.