
You can work with offcial effortlessly with the help of our online tool for PDF editing. Our team is dedicated to providing you the best possible experience with our editor by consistently adding new features and enhancements. With these improvements, using our tool becomes better than ever! Getting underway is simple! All that you should do is take the next simple steps directly below:
Step 1: Press the "Get Form" button above on this page to access our editor.
Step 2: With the help of our handy PDF file editor, it is possible to accomplish more than simply fill out blank fields. Express yourself and make your forms appear perfect with customized text incorporated, or tweak the file's original input to excellence - all comes with the capability to insert your personal images and sign it off.
When it comes to blanks of this specific document, here's what you should do:
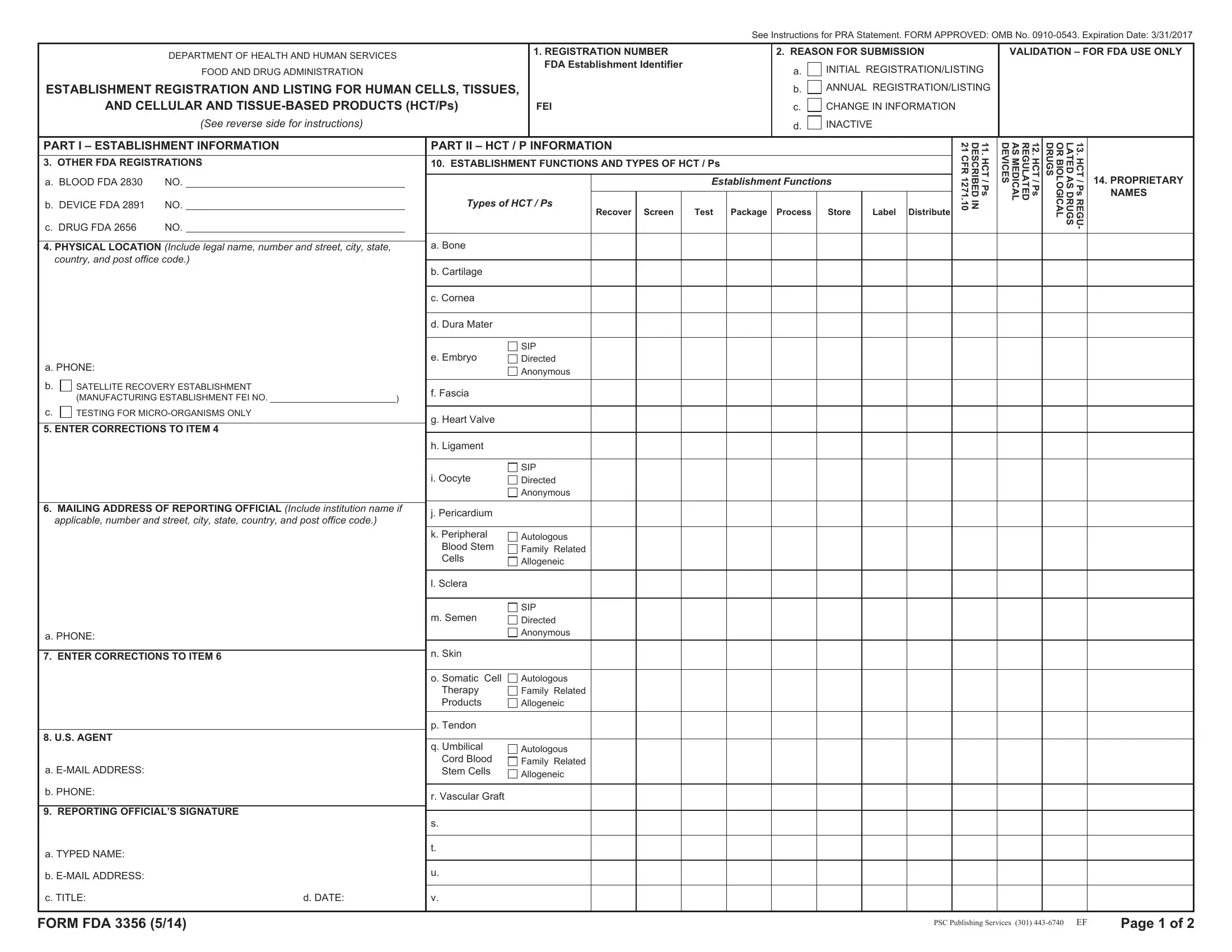
1. It's essential to complete the offcial accurately, thus be attentive when filling in the segments containing all of these blank fields:
2. Once this array of fields is complete, you're ready to include the required specifics in MAILING ADDRESS OF REPORTING, applicable number and street city, Autologous Family Related, SIP Directed Anonymous, j Pericardium, k Peripheral, Blood Stem Cells, l Sclera, m Semen, n Skin, a PHONE, ENTER CORRECTIONS TO ITEM, US AGENT, a EMAIL ADDRESS, and b PHONE so you're able to move forward to the third part.
Lots of people frequently get some points incorrect while filling out Autologous Family Related in this section. You need to go over what you enter right here.
Step 3: Always make sure that the information is accurate and then simply click "Done" to continue further. Join FormsPal now and immediately use offcial, all set for download. All modifications you make are saved , which means you can modify the file later if needed. FormsPal guarantees your data privacy by using a secure method that never saves or shares any personal information used in the form. Rest assured knowing your files are kept safe every time you use our editor!