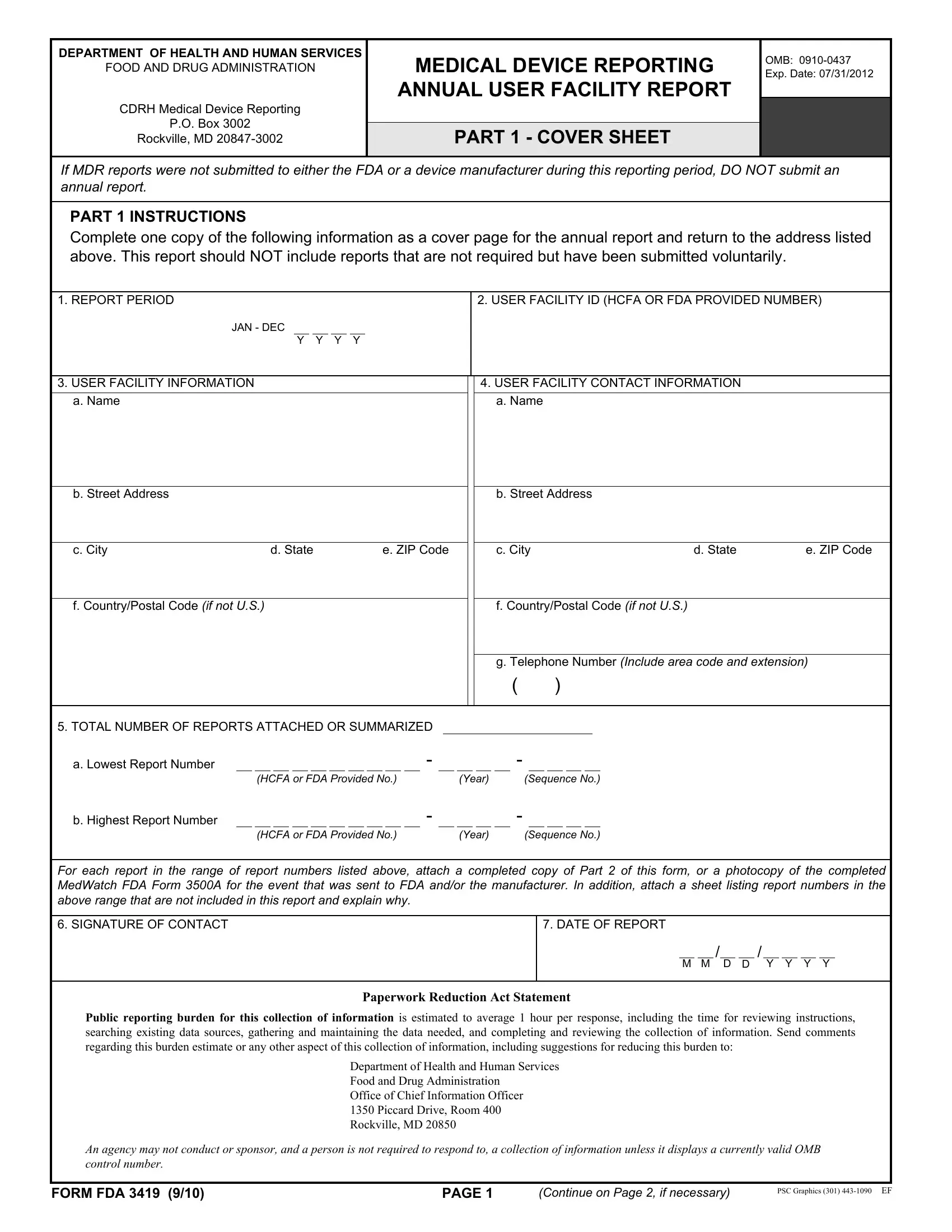
Healthcare facilities and professionals are well-acquainted with the multitude of documents and forms required to maintain compliance with federal regulations, one of which includes the FDA 3419 form. Issued by the Department of Health and Human Services' Food and Drug Administration, this form is a crucial element in the Medical Device Reporting (MDR) process. Annually, user facilities are required to submit a comprehensive report detailing incidents related to medical devices that have had significant adverse effects. The FDA 3419 form serves as a cover sheet and an organizational tool that guides the submission of these critical reports. Designed to streamline the process, the form requires specific information, such as user facility details, contact information, and a summary of events reported throughout the year, if any. Importantly, the directive clarifies that if no MDR reports were filed within the year, submitting an annual report is unnecessary, minimizing unnecessary paperwork. Furthermore, the form stipulates the inclusion of a range of report numbers, attaching a complete copy of Part 2 of the form, or a photocopy of the completed MedWatch FDA Form 3500A for each event reported to the FDA and/or manufacturer. Its structured format aids in ensuring that all pertinent information is provided efficiently and accurately, ultimately aiding the FDA in its mission to protect public health by monitoring medical device performance and responding to potential safety concerns.
| Question | Answer |
|---|---|
| Form Name | Form FDA 3419 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | fda form 3419 annual user facility report, form fda 3419, fda form 3419, form 3419 |
