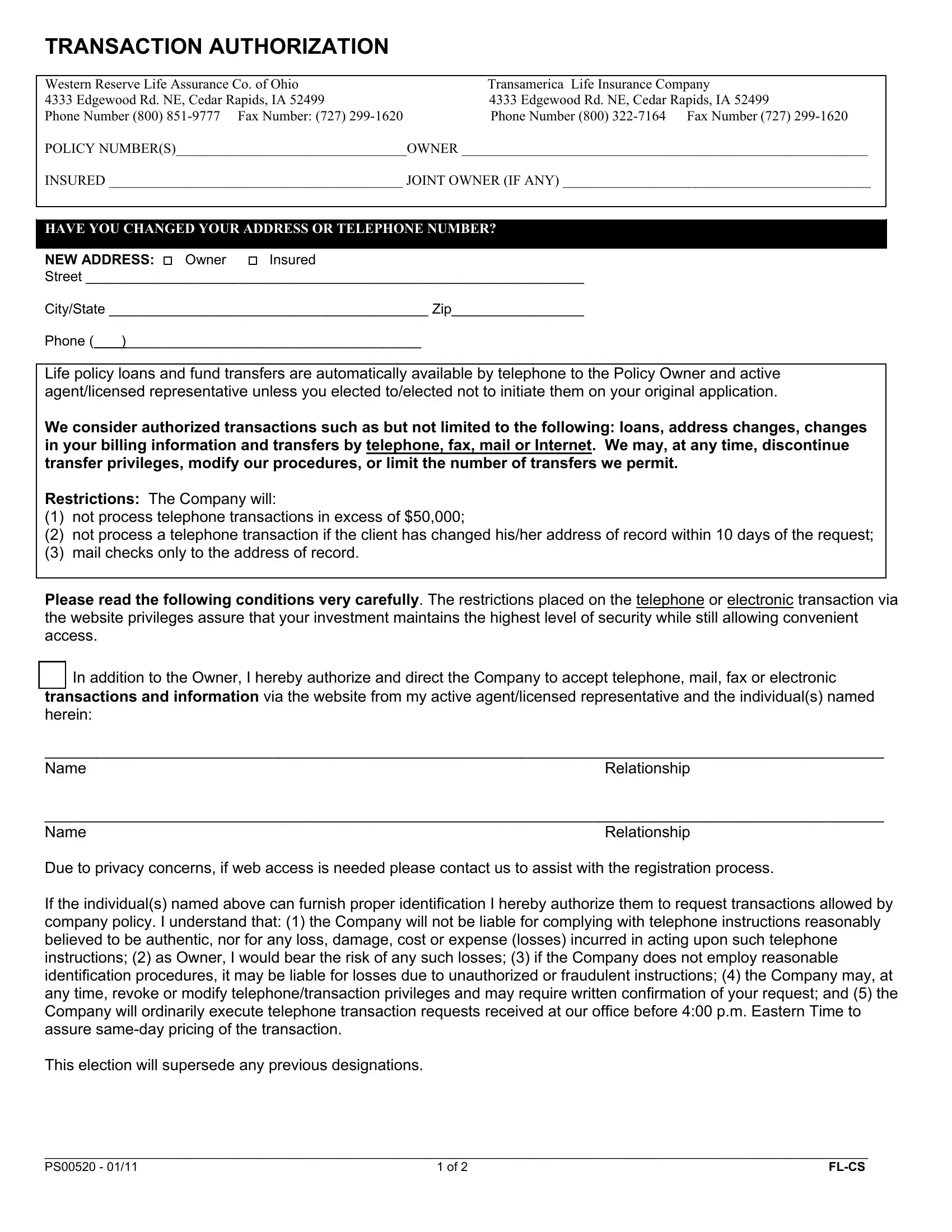
TRANSACTION AUTHORIZATION
Western Reserve Life Assurance Co. of Ohio |
Transamerica Life Insurance Company |
4333 Edgewood Rd. NE, Cedar Rapids, IA 52499 |
|
4333 Edgewood Rd. NE, Cedar Rapids, IA 52499 |
Phone Number (800) 851-9777 Fax Number: (727) 299-1620 |
Phone Number (800) 322-7164 Fax Number (727) 299-1620 |
POLICY NUMBER(S)_________________________________OWNER __________________________________________________________
INSURED __________________________________________ JOINT OWNER (IF ANY) ____________________________________________
HAVE YOU CHANGED YOUR ADDRESS OR TELEPHONE NUMBER?
NEW ADDRESS: Owner |
Insured |
Street ________________________________________________________________
City/State _________________________________________ Zip_________________
Phone ( )______________________________________
Life policy loans and fund transfers are automatically available by telephone to the Policy Owner and active agent/licensed representative unless you elected to/elected not to initiate them on your original application.
We consider authorized transactions such as but not limited to the following: loans, address changes, changes in your billing information and transfers by telephone, fax, mail or Internet. We may, at any time, discontinue transfer privileges, modify our procedures, or limit the number of transfers we permit.
Restrictions: The Company will:
(1)not process telephone transactions in excess of $50,000;
(2)not process a telephone transaction if the client has changed his/her address of record within 10 days of the request;
(3)mail checks only to the address of record.
Please read the following conditions very carefully. The restrictions placed on the telephone or electronic transaction via the website privileges assure that your investment maintains the highest level of security while still allowing convenient access.
In addition to the Owner, I hereby authorize and direct the Company to accept telephone, mail, fax or electronic transactions and information via the website from my active agent/licensed representative and the individual(s) named herein:
_________________________________________________________________________________________________
NameRelationship
_________________________________________________________________________________________________
Due to privacy concerns, if web access is needed please contact us to assist with the registration process.
If the individual(s) named above can furnish proper identification I hereby authorize them to request transactions allowed by company policy. I understand that: (1) the Company will not be liable for complying with telephone instructions reasonably believed to be authentic, nor for any loss, damage, cost or expense (losses) incurred in acting upon such telephone instructions; (2) as Owner, I would bear the risk of any such losses; (3) if the Company does not employ reasonable identification procedures, it may be liable for losses due to unauthorized or fraudulent instructions; (4) the Company may, at any time, revoke or modify telephone/transaction privileges and may require written confirmation of your request; and (5) the Company will ordinarily execute telephone transaction requests received at our office before 4:00 p.m. Eastern Time to assure same-day pricing of the transaction.
This election will supersede any previous designations.
_______________________________________________________________________________________________________________________
PS00520 - 01/11 |
1 of 2 |
FL-CS |
Please read the following very carefully to DISABLE a current authorized privilege.
(only complete this section if you want to disable a current authorized person’s access to your policy)
DISABLE ONLY current telephone/transaction authorization privileges for:
(DO NOT check this box if you are giving the person listed on the previous section authorization)
Note: Your active Servicing Representative will still have access to view your policy. If you want to remove your agent, please submit your request in a written Letter of Instruction.
|
All (except owner) |
|
Active agent/licensed representative |
|
Other: _______________________________________________________________________________________ |
|
Name |
|
Relationship |
|
|
The transfer privilege under the Policy is not intended to serve as a vehicle for short-term or frequent transfers. The Policy does not permit market timing/frequent transfers. As described above, frequent transfers among investment option portfolios disrupt portfolio management in the underlying mutual fund and tend to drive fund expenses higher. We reserve the right to limit or revoke your transfer privileges and/or may not accept future premium payments from you if you engage in frequent transfer activity. You may only transfer values between subaccounts in the Transamerica Series Trust or the Fidelity Variable Insurance Products fund by sending us your written request, with original signature authorizing each transfer, through standard United States postal delivery (no overnight or other priority delivery service).
Signature of Owner _____________________________________________________________ Date ________________________
______________________________________________________________
Print Name / Title (POA, Trustee, Guardian, etc..)
Signature of Spouse or Joint Owner (if any) __________________________________________ Date ________________________
______________________________________________________________
Print Name / Title (POA, Trustee, Guardian, etc..)
Signature of Authorized Person named____________________________________________________ Date ______________________
______________________________________________________________
Print Name
Signature of Authorized Person named____________________________________________________ Date ______________________
______________________________________________________________
Print Name
PLEASE NOTE: If you reside in one of the following community property jurisdictions (AZ, CA, ID, LA,NM, NV, TX, WA, WI, Puerto Rico and Guam), you may wish to consult with your legal or tax advisor prior to making changes to your policy.
This request may be mailed or faxed.
___________________________________________________________________________________________________________________
PS00520 - 01/11 |
2 of 2 |
FL-CS |