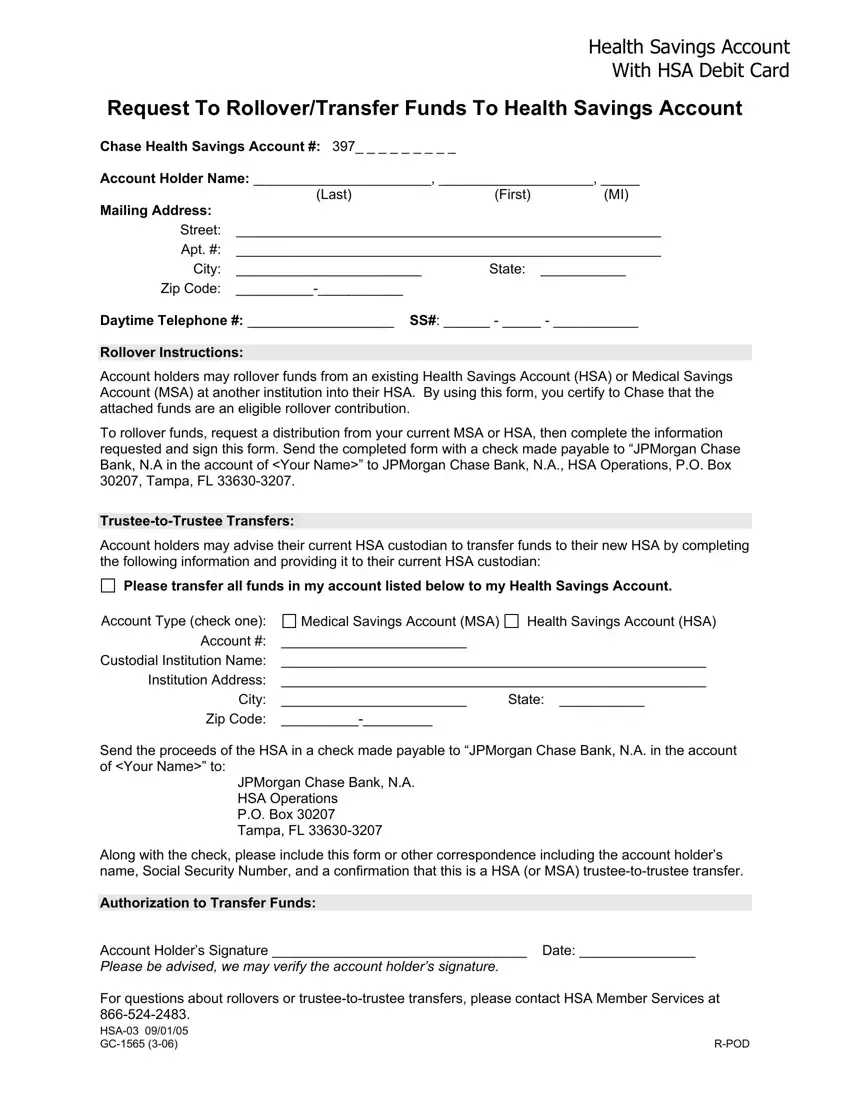
In the landscape of healthcare financing, the flexibility and advantages offered by Health Savings Accounts (HSAs) stand out as a crucial component. The GC 1565 form plays a pivotal role in this ecosystem, serving as a formal request for individuals wishing to rollover or transfer funds to their HSA with Chase, a process that underscores the fluidity and user-centric nature of managing these accounts. This form caters to both rollovers from existing HSAs or Medical Savings Accounts (MSAs) and facilitates trustee-to-trustee transfers, offering a streamlined pathway for account holders to consolidate or shift their healthcare savings. It requires detailed information, including the account holder's name, Social Security Number, and the specifics of the transferring and receiving accounts to ensure a smooth transaction. Additionally, the form harbors critical instructions for both the account holder and the custodian of their prior HSA or MSA, including making a check payable to “JPMorgan Chase Bank, N.A. in the account of [Your Name],” thereby crystallizing the transfer or rollover. The form not only exemplifies the procedural aspect of managing HSAs but also reflects the broader commitment to providing accessible healthcare savings mechanisms that empower individuals to manage their health finance with autonomy and precision.
| Question | Answer |
|---|---|
| Form Name | Form Gc 1565 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | certify, HSA-03, GC-1565, Custodial |
Health Savings Account
With HSA Debit Card
Request To Rollover/Transfer Funds To Health Savings Account
Chase Health Savings Account #: 397_ _ _ _ _ _ _ _ _
Account Holder Name: _______________________, ____________________, _____
|
(Last) |
(First) |
(MI) |
Mailing Address: |
|
|
|
Street: |
_______________________________________________________ |
||
Apt. #: |
_______________________________________________________ |
||
City: |
________________________ |
State: |
___________ |
Zip Code: |
|
|
|
Daytime Telephone #: ___________________ SS#: ______ - _____ - ___________
Rollover Instructions:
Account holders may rollover funds from an existing Health Savings Account (HSA) or Medical Savings Account (MSA) at another institution into their HSA. By using this form, you certify to Chase that the attached funds are an eligible rollover contribution.
To rollover funds, request a distribution from your current MSA or HSA, then complete the information requested and sign this form. Send the completed form with a check made payable to “JPMorgan Chase Bank, N.A in the account of <Your Name>” to JPMorgan Chase Bank, N.A., HSA Operations, P.O. Box 30207, Tampa, FL
Account holders may advise their current HSA custodian to transfer funds to their new HSA by completing the following information and providing it to their current HSA custodian:
Please transfer all funds in my account listed below to my Health Savings Account.
Account Type (check one): |
Medical Savings Account (MSA) |
Health Savings Account (HSA) |
Account #: |
________________________ |
|
Custodial Institution Name: |
_______________________________________________________ |
|
Institution Address: |
_______________________________________________________ |
|
City: |
________________________ |
State: ___________ |
Zip Code: |
|
|
Send the proceeds of the HSA in a check made payable to “JPMorgan Chase Bank, N.A. in the account of <Your Name>” to:
JPMorgan Chase Bank, N.A. HSA Operations
P.O. Box 30207 Tampa, FL
Along with the check, please include this form or other correspondence including the account holder’s name, Social Security Number, and a confirmation that this is a HSA (or MSA)
Authorization to Transfer Funds:
Account Holder’s Signature _________________________________ Date: _______________
Please be advised, we may verify the account holder’s signature.
For questions about rollovers or
|
|
