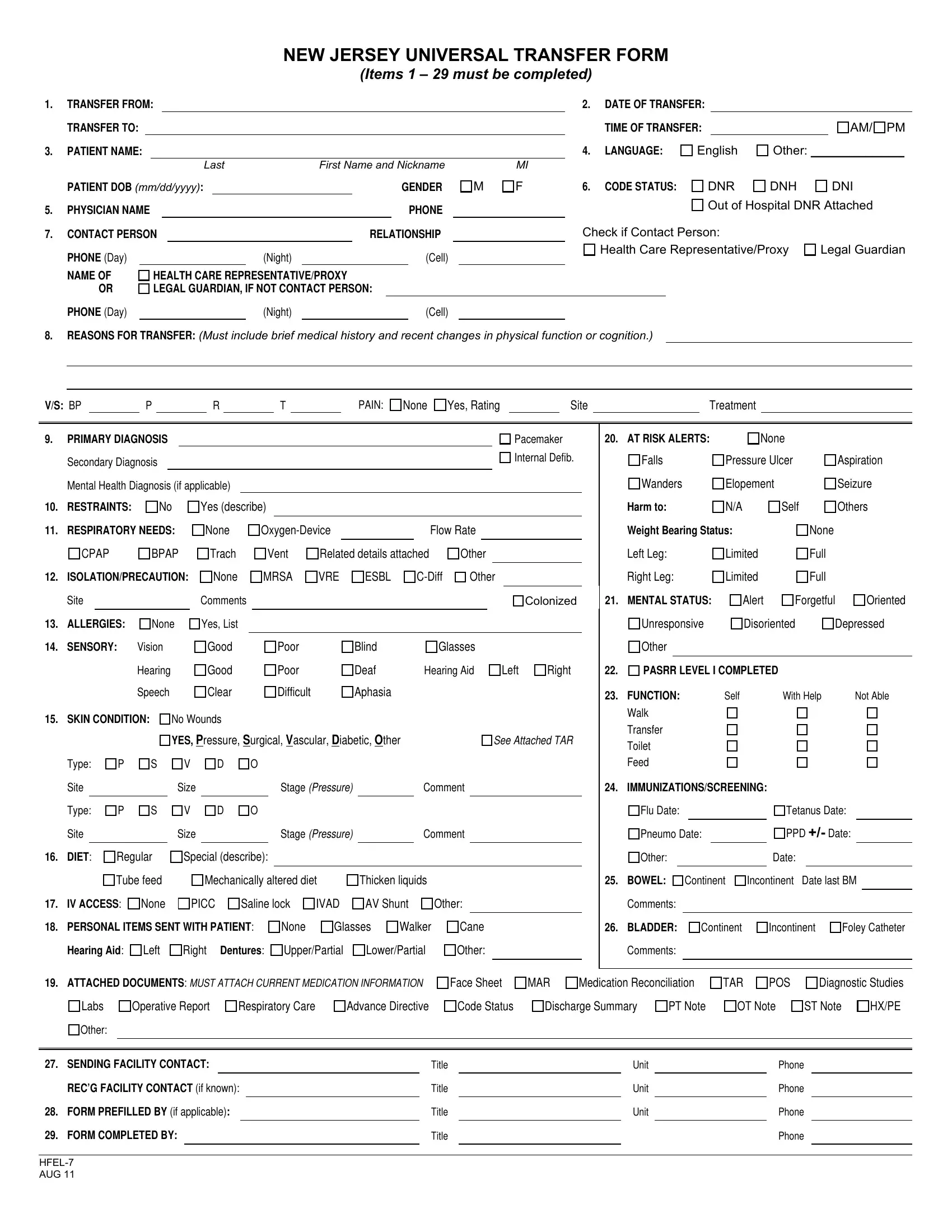
The New Jersey Universal Transfer Form, known as the HFEL-7, serves as a comprehensive document meant to streamline and secure the process of transferring a patient between healthcare facilities. This crucial piece of documentation covers a wide array of information necessary for ensuring continuity of care and minimizing errors during transitions. The form mandates the inclusion of basic yet vital details such as the transfer points, timing, and patient demographics like name, date of birth, and gender. It extends to encompass more specific health-related information, including the patient's code status, primary and secondary diagnoses, respiratory needs, and potential isolation precautions. Furthermore, the form delves into the patient's current condition and care requirements, touching on aspects like allergies, sensory impairments, skin condition, diet, and functional status. It also provides sections for noting personal items sent with the patient, current medications, attached documents for health history, and contact information for the sending and receiving facilities. The meticulous nature of the HFEL-7 form highlights its role in not just providing a snapshot of a patient's health status but also ensuring that receiving facilities are fully informed and optimally prepared to continue providing appropriate and effective care.
| Question | Answer |
|---|---|
| Form Name | Form Hfel 7 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Defib, nj universal transfer form, new jersey universal transfer form, C-Diff |
NEW JERSEY UNIVERSAL TRANSFER FORM
(Items 1 – 28 must be completed)
1. |
TRANSFER FROM: |
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
DATE OF TRANSFER: |
|
|
|
|
|||||
|
TRANSFER TO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TIME OF TRANSFER: |
|
|
|
AM/ PM |
||||
3. |
PATIENT NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
LANGUAGE: |
English |
Other: ____________ |
|||||||
|
|
|
|
|
|
|
Last |
|
First Name and Nickname |
|
|
MI |
|
|
|
|
|
|
|
|
|||||
|
PATIENT DOB (mm/dd/yyyy): |
|
|
|
|
GENDER |
|
M |
F |
6. |
CODE STATUS: |
DNR |
DNH |
|
DNI |
||||||||||
5. |
PHYSICIAN NAME |
|
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
Out of Hospital DNR Attached |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
7. |
CONTACT PERSON |
|
|
RELATIONSHIP |
|
|
|
Check if Contact Person: |
|
|
|
||||||||||||||
|
PHONE (Day) |
|
|
|
|
|
(Night) |
|
|
|
|
(Cell) |
|
|
|
|
Health Care Representative/Proxy |
Legal Guardian |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
NAME OF |
HEALTH CARE REPRESENTATIVE/PROXY |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
OR |
LEGAL GUARDIAN, IF NOT CONTACT PERSON: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
PHONE (Day) |
|
|
|
|
|
(Night) |
|
|
|
|
(Cell) |
|
|
|
|
|
|
|
|
|
|
|
||
8.REASONS FOR TRANSFER: (Must include brief medical history and recent changes in physical function or cognition.)
V/S: BP |
|
P |
|
R |
|
T |
|
PAIN: |
None
Yes, Rating |
|
Site |
|
Treatment |
9. |
PRIMARY DIAGNOSIS |
|
|
|
|
|
|
|
|
|
|
|
|
Pacemaker |
|||
|
Secondary Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
Internal Defib. |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Mental Health Diagnosis (if applicable) |
|
|
|
|
|
|
|
|
|
|
|
|||||
10. |
RESTRAINTS: |
No |
Yes (describe) |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||
11. |
RESPIRATORY NEEDS: |
None |
|
Flow Rate |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CPAP |
BPAP |
Trach |
Vent |
Related details attached |
Other |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
12. |
ISOLATION/PRECAUTION: |
None |
MRSA |
VRE |
ESBL |
Other |
|||||||||||
|
Site |
|
|
|
Comments |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Colonized |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. |
AT RISK ALERTS: |
|
None |
|
Falls |
Pressure Ulcer |
|
|
Wanders |
Elopement |
|
|
Harm to: |
N/A |
Self |
|
Weight Bearing Status: |
|
|
|
Left Leg: |
Limited |
|
|
Right Leg: |
Limited |
|
21. |
MENTAL STATUS: |
|
|
Aspiration
Seizure
Others
None
Full
Full
13. |
ALLERGIES: |
None |
Yes, List |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. |
SENSORY: |
Vision |
|
Good |
Poor |
Blind |
Glasses |
|
|
|
|
Hearing |
|
Good |
Poor |
Deaf |
Hearing Aid |
Left |
Right |
|
|
Speech |
|
Clear |
Difficult |
Aphasia |
|
|
|
15. |
SKIN CONDITION: |
No Wounds |
|
|
|
|
|
||
Alert |
|
Forgetful |
Oriented |
|
Unresponsive |
|
Disoriented |
Depressed |
|
Other |
|
|
|
|
|
|
|
|
|
22. FUNCTION: |
Self |
With Help |
Not Able |
|
Walk
Transfer
Type:
Site
Type:
Site
16. DIET:
YES, Pressure, Surgical, Vascular, Diabetic, Other
P |
S |
V |
D |
O |
|
|
|
|
|
Size |
|
|
Stage (PRESSURE) |
|
Comment |
|
|
|
|
|
|
|
|
P |
S |
V |
D |
O |
|
|
|
|
|
Size |
|
|
Stage (PRESSURE) |
|
Comment |
|
|
|
|
|
|
||
Regular |
Special (describe): |
|
|
||||
SEE ATTACHED TAR
Toilet
Feed
23. IMMUNIZATIONS/SCREENING:
Flu Date: |
Tetanus Date: |
|||||
|
|
|
|
|
|
|
Pneumo Date: |
PPD +/- Date: |
|||||
|
|
|
|
|
|
|
Other: |
Date: |
|||||
|
|
|
|
|
|
|
|
Tube feed |
Mechanically altered diet |
Thicken liquids |
|
|
|
|||||
17. |
IV ACCESS: |
None |
PICC |
Saline lock |
IVAD |
AV Shunt |
Other: |
||||
|
|
|
|
|
|
|
|
||||
18. |
PERSONAL ITEMS SENT WITH PATIENT: |
None |
Glasses |
Walker |
Cane |
||||||
|
Hearing Aid: |
Left |
Right |
Dentures: |
Upper/Partial |
Lower/Partial |
Other: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
24.BOWEL: Continent Incontinent Date last BM Comments:
25. BLADDER: |
Continent |
Incontinent |
Foley Catheter |
Comments:
19.ATTACHED DOCUMENTS: MUST ATTACH CURRENT MEDICATION INFORMATION
Labs |
Operative Report |
Respiratory Care |
Advance Directive |
Other:
Face Sheet Code Status
MAR |
Medication Reconciliation |
|
Discharge Summary |
PT Note |
|
TAR POS
OT Note
Diagnostic Studies
ST Note |
HX/PE |
26. |
SENDING FACILITY CONTACT: |
|
Title |
|
Unit |
|
Phone |
|||
|
REC’G FACILITY CONTACT (if known): |
Title |
|
Unit |
|
Phone |
||||
|
|
|
|
|
|
|
|
|
|
|
27. |
FORM PREFILLED BY (if applicable): |
Title |
|
Unit |
|
Phone |
||||
|
|
|
|
|
|
|
|
|
||
28. |
FORM COMPLETED BY: |
|
Title |
|
|
|
Phone |
|||