Understanding the HR-BEN-031A form is crucial for retirees seeking Medicare Part B reimbursement. At its core, the form is designed to facilitate the process of applying for a refund of Medicare Part B premiums for retirees who fulfill set conditions. Eligibility hinges on a combination of factors including receiving a pension from specific New York City entities, enrollment in a qualifying health plan, and having paid Medicare Part B premiums. With sections covering personal information, declarations of truthfulness, and authorization for the Social Security Administration to release necessary data, the form serves as a comprehensive tool for retirees. Moreover, the inclusion of instructions for submission, eligibility criteria, and the importance of accompanying documents like the Medicare card and Form SSA-1099 emphasize the form's role in ensuring accurate and timely reimbursements. Completing and submitting the HR-BEN-031A is a straightforward process, detailed within the document, offering clear guidance on obtaining reimbursements, which are typically processed within three months after receipt of a completed application. This form exemplifies the administrative steps retirees must navigate to secure refunds, underscoring the importance of adhering to specified requirements and maintaining open communication with the MTA Business Service Center for any changes or inquiries.
| Question | Answer |
|---|---|
| Form Name | Form Hr Ben 031A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | E-mail, HR-BEN-031a, MTA, NYCERS |
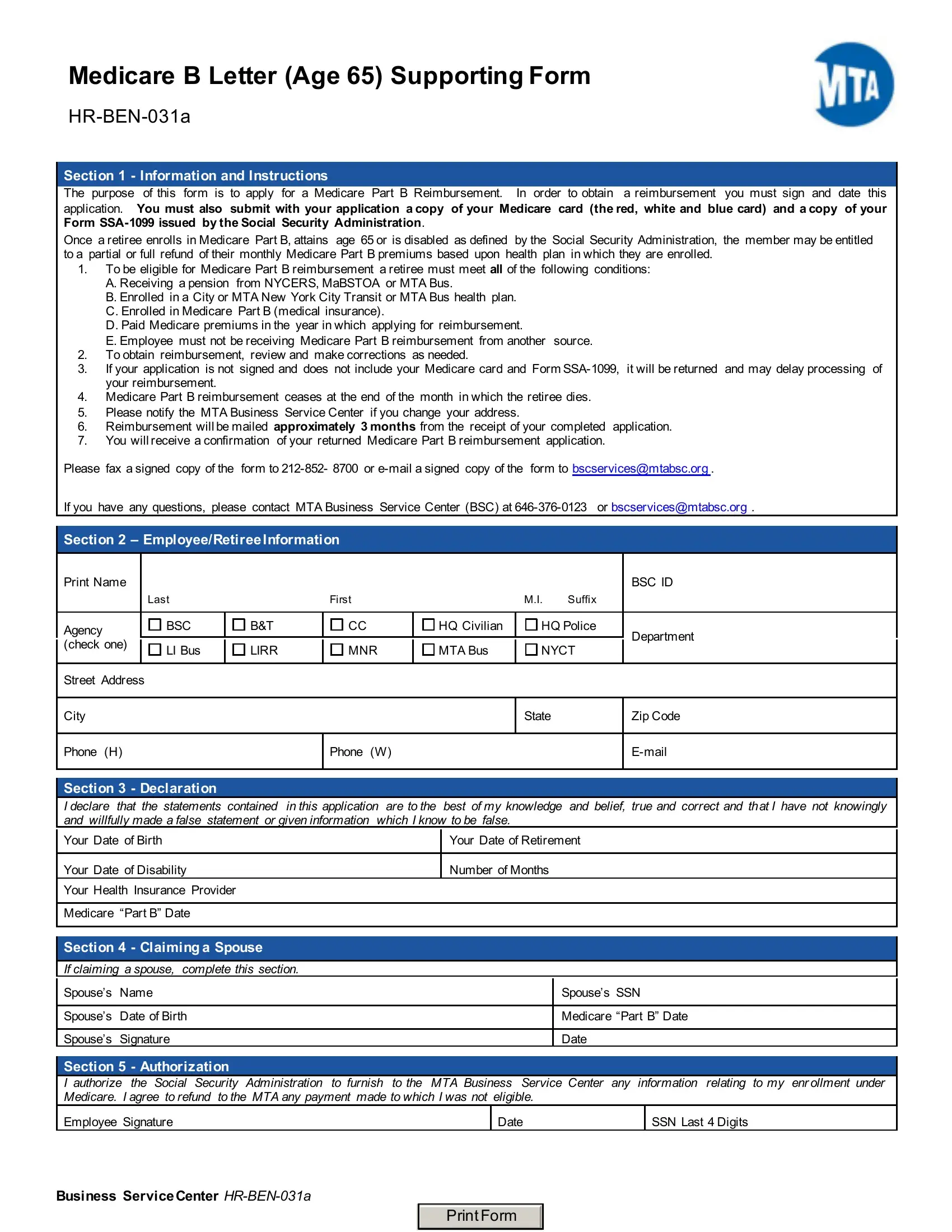
Medicare B Letter (Age 65) Supporting Form
Section 1 - Information and Instructions
The purpose of this form is to apply for a Medicare Part B Reimbursement. In order to obtain a reimbursement you must sign and date this
application. You must also submit with your application a copy of your Medicare card (the red, white and blue card) and a copy of your Form
Once a retiree enrolls in Medicare Part B, attains age 65 or is disabled as defined by the Social Security Administration, the member may be entitled to a partial or full refund of their monthly Medicare Part B premiums based upon health plan in which they are enrolled.
1.To be eligible for Medicare Part B reimbursement a retiree must meet all of the following conditions:
A.Receiving a pension from NYCERS, MaBSTOA or MTA Bus.
B.Enrolled in a City or MTA New York City Transit or MTA Bus health plan.
C.Enrolled in Medicare Part B (medical insurance).
D.Paid Medicare premiums in the year in which applying for reimbursement.
E.Employee must not be receiving Medicare Part B reimbursement from another source.
2.To obtain reimbursement, review and make corrections as needed.
3.If your application is not signed and does not include your Medicare card and Form
4.Medicare Part B reimbursement ceases at the end of the month in which the retiree dies.
5.Please notify the MTA Business Service Center if you change your address.
6.Reimbursement will be mailed approximately 3 months from the receipt of your completed application.
7.You will receive a confirmation of your returned Medicare Part B reimbursement application.
Please fax a signed copy of the form to
If you have any questions, please contact MTA Business Service Center (BSC) at
Section 2 – Employee/RetireeInformation
|
Print Name |
|
|
|
|
|
|
|
|
|
|
|
|
BSC ID |
|
|
|
Last |
|
|
|
First |
|
|
|
M.I. |
Suffix |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Agency |
|
BSC |
|
B&T |
|
CC |
|
HQ Civilian |
|
HQ Police |
|
Department |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
(check one) |
|
LI Bus |
|
LIRR |
|
MNR |
|
MTA Bus |
|
NYCT |
|
||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone (H) |
|
|
|
|
Phone (W) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Section 3 - Declaration
|
I declare that the statements contained |
in this application are to the best of my knowledge and belief, true and correct and that I have not knowingly |
||
|
and willfully made a false statement or given information which I know to be false. |
|||
|
Your Date of Birth |
|
Your Date of Retirement |
|
|
|
|
||
|
|
|
|
|
|
Your Date of Disability |
|
Number of Months |
|
|
Your Health Insurance Provider |
|
|
|
|
|
|
|
|
|
Medicare “Part B” Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
Section 4 - Claiming a Spouse
If claiming a spouse, complete this section.
Spouse’s |
Name |
Spouse’s SSN |
|
|
|
Spouse’s |
Date of Birth |
Medicare “Part B” Date |
|
|
|
Spouse’s |
Signature |
Date |
Section 5 |
- Authorization |
|
|
|
|
I authorize |
the Social Security Administration |
to furnish to the MTA Business Service Center |
any information relating to my enrollment under |
||
Medicare. I agree to refund to the MTA any payment made to which I was not eligible. |
|
|
|||
Employee Signature |
|
Date |
|
SSN Last 4 Digits |
|
Business ServiceCenter
PrintForm