
You can certainly get forms applying our PDF editor. Changing the hud 52665 form form is not difficult if you keep up with these actions:
Step 1: At first, pick the orange "Get form now" button.
Step 2: You're now on the document editing page. You may edit, add information, highlight particular words or phrases, put crosses or checks, and insert images.
Fill out the hud 52665 form PDF by providing the text necessary for each individual section.
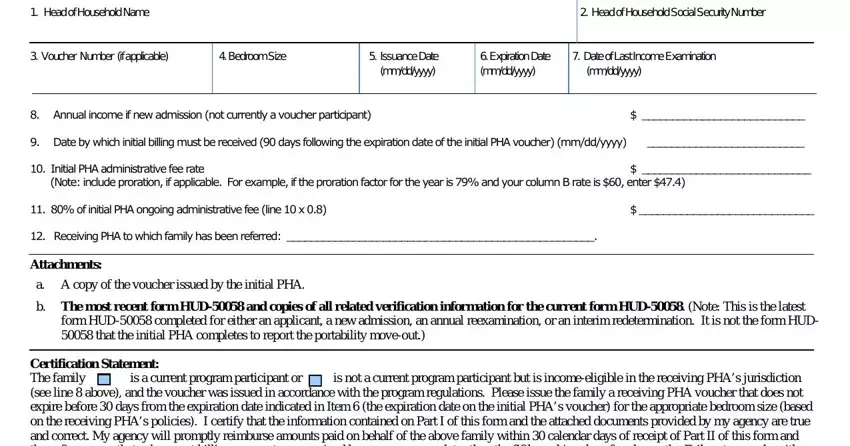
Jot down the details in Name, of, Certifying, PHA, Official Signature, Initial, PHA, Contact, Name Phone, Number Email, Form, Submission, Date, mm, dd, yyyy and form, HUD
In the Head, of, Household, Name Head, of, Household, Social, Security, Number HAP, Contract, Number, if, applicable Receiving, PHA, administrative, fee, rate Name, of, Certifying, PHA, Official Signature, Receiving, PHA, Contact, Name Phone, Number Email, and Form, Submission, Date, mm, dd, yyyy box, describe the key data.
Inside of box annual, recertification interim, special, recertification and change, in, payment, standard identify the rights and obligations.
Complete the form by analyzing all these sections: other, specify Comments, continued, on, separate, page, Yes and form, HUD
Step 3: Choose the button "Done". The PDF document can be transferred. You will be able obtain it to your pc or send it by email.
Step 4: You may create duplicates of your form tostay clear of all of the potential future issues. You need not worry, we don't distribute or track your information.
