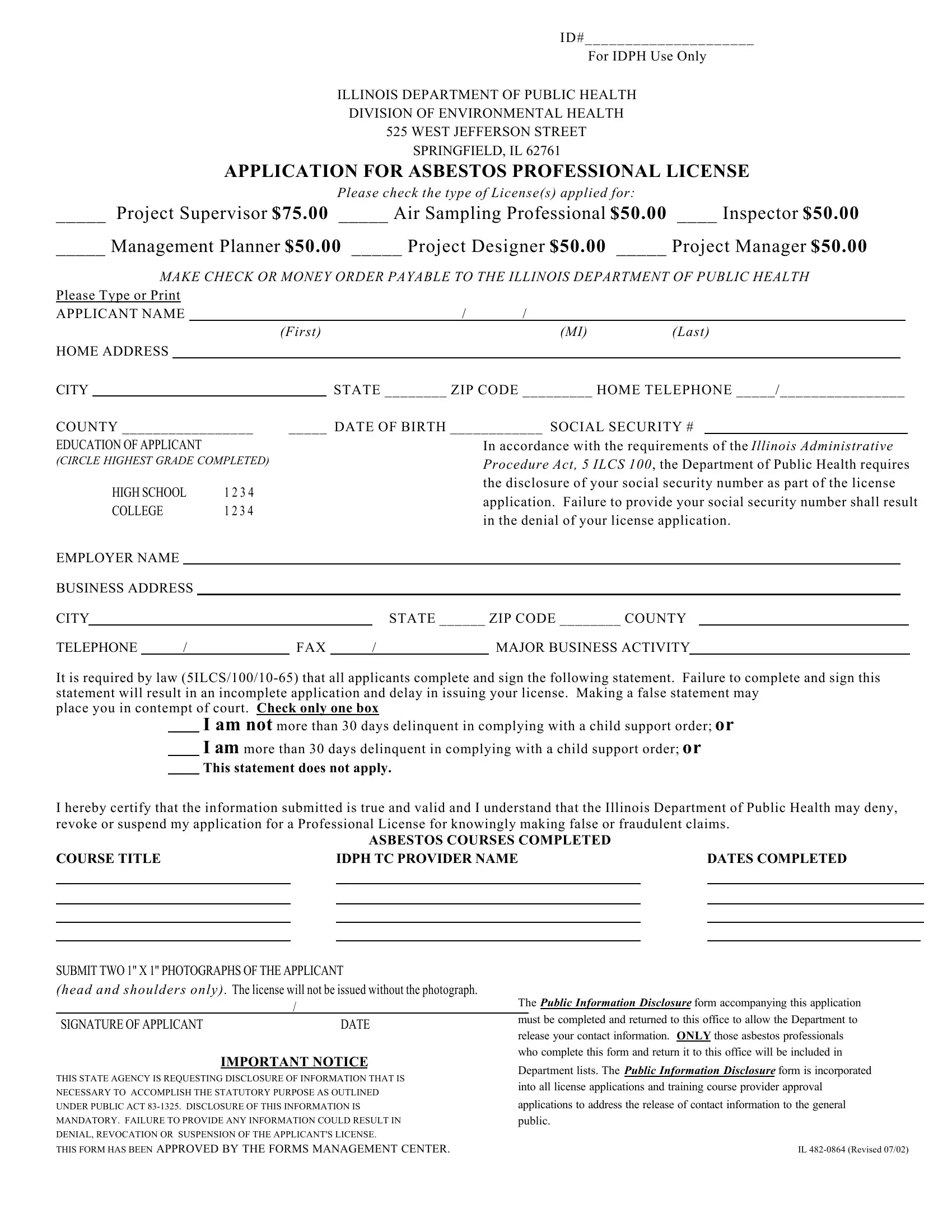
Professionals seeking to navigate the complex regulations surrounding asbestos handling and removal in Illinois will find the IL 482 0864 form to be an essential step in legitimizing their qualifications and ensuring compliance with state guidelines. Issued by the Illinois Department of Public Health (IDPH) Division of Environmental Health, this form serves as an application for various asbestos professional licenses, including Project Supervisor, Air Sampling Professional, Inspector, Management Planner, Project Designer, and Project Manager, each requiring a specified fee. Applicants are asked to provide detailed personal and educational information, alongside their social security number as mandated by the Illinois Administrative Procedure Act, 5 ILCS 100, for the processing of the application. The form also addresses legal compliance regarding child support orders and emphasizes the importance of honesty in the submission of information, underlining the severe consequences for making false statements. Furthermore, it includes sections for detailed experience related to the type of license applied for, specifying that experience be listed in hours and allowing for additional sheets to detail extensive experience. The requirement of submitting two 1" x 1" photographs underscores the form's attention to detail and the importance placed on the accuracy and completeness of the application. With stringent requirements and a comprehensive approach to information gathering, the IL 482 0864 form represents a crucial hurdle for professionals aiming to contribute to asbestos management and removal projects within Illinois safely and legally.
| Question | Answer |
|---|---|
| Form Name | Form Il 482 0864 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | illinois asbestos license application, illinois asbestos license lookup, illinois licensed asbestos abatement contractors application, idph asbestos professional license renewal |
ID#_____________________
For IDPH Use Only
ILLINOIS DEPARTMENT OF PUBLIC HEALTH DIVISION OF ENVIRONMENTAL HEALTH 525 WEST JEFFERSON STREET SPRINGFIELD, IL 62761
APPLICATION FOR ASBESTOS PROFESSIONAL LICENSE
Please check the type of License(s) applied for:
_____ Project Supervisor $75.00 _____ Air Sampling Professional $50.00 ____ Inspector $50.00
_____ Management Planner $50.00 |
_____ Project Designer $50.00 |
_____ Project Manager $50.00 |
||
MAKE CHECK OR MONEY ORDER PAYABLE TO THE ILLINOIS DEPARTMENT OF PUBLIC HEALTH |
||||
Please Type or Print |
|
|
|
|
APPLICANT NAME |
/ |
/ |
|
|
|
(First) |
|
(MI) |
(Last) |
HOME ADDRESS
CITY
COUNTY _________________
EDUCATION OF APPLICANT
(CIRCLE HIGHEST GRADE COMPLETED)
HIGH SCHOOL |
1 2 3 4 |
COLLEGE |
1 2 3 4 |
STATE ________ ZIP CODE _________ HOME TELEPHONE _____/________________
_____ DATE OF BIRTH ____________ SOCIAL SECURITY #
In accordance with the requirements of the Illinois Administrative Procedure Act, 5 ILCS 100, the Department of Public Health requires the disclosure of your social security number as part of the license application. Failure to provide your social security number shall result in the denial of your license application.
EMPLOYER NAME |
|
|
|
|
|
|
|
|
|
|
||
BUSINESS ADDRESS |
|
|
|
|
|
|
|
|
|
|||
CITY |
|
|
|
|
|
|
STATE ______ ZIP CODE ________ COUNTY |
|
|
|||
TELEPHONE |
|
/ |
|
FAX |
|
/ |
|
MAJOR BUSINESS ACTIVITY |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
It is required by law
place you in contempt of court. Check only one box
I am not more than 30 days delinquent in complying with a child support order; or
I am more than 30 days delinquent in complying with a child support order; or
This statement does not apply.
I hereby certify that the information submitted is true and valid and I understand that the Illinois Department of Public Health may deny, revoke or suspend my application for a Professional License for knowingly making false or fraudulent claims.
ASBESTOS COURSES COMPLETED
COURSE TITLE |
|
IDPH TC PROVIDER NAME |
|
DATES COMPLETED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUBMIT TWO 1" X 1" PHOTOGRAPHS OF THE APPLICANT
(head and shoulders only). The license will not be issued without the photograph.
/
SIGNATURE OF APPLICANT |
DATE |
IMPORTANT NOTICE
THIS STATE AGENCY IS REQUESTING DISCLOSURE OF INFORMATION THAT IS NECESSARY TO ACCOMPLISH THE STATUTORY PURPOSE AS OUTLINED UNDER PUBLIC ACT
THIS FORM HAS BEEN APPROVED BY THE FORMS MANAGEMENT CENTER.
The PUBLIC INFORMATION DISCLOSURE form accompanying this application must be completed and returned to this office to allow the Department to release your contact information. ONLY those asbestos professionals who complete this form and return it to this office will be included in Department lists. The PUBLIC INFORMATION DISCLOSURE form is incorporated into all license applications and training course provider approval applications to address the release of contact information to the general public.
IL
COMPLETE THIS PORTION OF THE APPLICATION IN DETAIL
GIVE INFORMATION RELATED TO TYPE OF LICENSE
Experience shall be listed in hours.
Attach additional sheets listing experience, if necessary.
Employer |
|
|
|
|
Job Title |
|
|
|
|
|
|
|
|
||||
Address |
|
|
|
|
|
Supervisor |
|
|
|
|
|
|
|
||||
City |
|
|
|
|
|
Telephone |
|
/ |
|
|
|
|
|
|
|||
State |
|
Zip |
Dates of Employment |
/ |
To |
/ |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
(mo) |
(yr) |
|
(mo) |
|
|
(yr) |
Duties & Responsibilities
Project Name |
# of Hours |
|
|
Employer |
|
|
|
|
|
Job Title |
|
|
|
|
|
|
|
|
||||
Address |
|
|
|
|
|
|
Supervisor |
|
|
|
|
|
|
Telephone |
/ |
|||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
State |
|
Zip |
|
Dates of Employment |
/ |
To |
/ |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
(mo) |
(yr) |
|
(mo) |
|
(yr) |
|
|
Duties & Responsibilities
Project Name |
# of Hours |
|
|
Employer |
|
|
|
|
|
Job Title |
|
|
|
|
|
|
|
|
||||
Address |
|
|
|
|
|
|
Supervisor |
|
|
|
|
|
|
Telephone |
/ |
|||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
State |
|
Zip |
|
Dates of Employment |
/ |
To |
/ |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
(mo) |
(yr) |
|
(mo) |
|
(yr) |
|
|
Duties & Responsibilities
Project Name |
# of Hours |
|
|