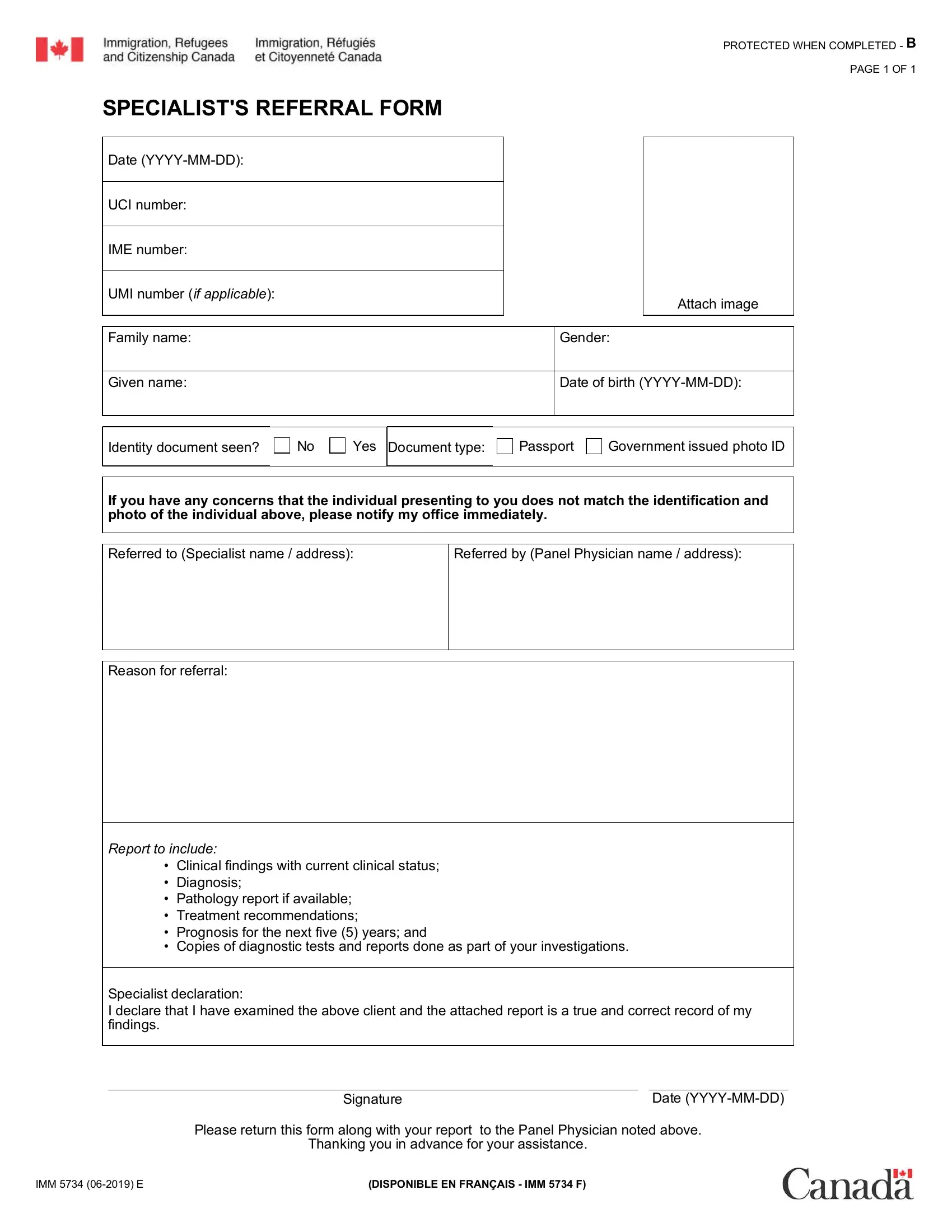
Navigating the complexities of immigration processes often involves dealing with various forms, one of which is the IMM 5734 form, also known as the Specialist's Referral Form. This document plays a critical role within the medical examination procedure for individuals seeking entry into a new country. The form contains several sections, starting with the individual's personal information, including the date, UCI (Unique Client Identifier), IME (Immigration Medical Examination), and UMI numbers, along with their full name, date of birth, and gender. It also requires confirmation of the identity document provided, such as a passport or government-issued photo ID, ensuring the person presenting the form matches the identification. What makes this form essential is its purpose: it's used by panel physicians to refer individuals to specialists. These referrals may occur due to the need for further assessment of a medical condition identified during the initial health screening. Specialists are then required to provide a detailed report that includes clinical findings, a diagnosis, any available pathology reports, treatment recommendations, a prognosis for the next five years, and copies of diagnostic tests and examinations. The form concludes with a declaration by the specialist, affirming the accuracy of the provided information. Completing and returning this form to the referring panel physician is crucial for ensuring the thorough assessment of an applicant's health status, which is a vital component of the immigration process.
| Question | Answer |
|---|---|
| Form Name | Form Imm 5734 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | canada imm 5734e pdf en francais, canada visa application, canadian visa application form pdf, canada visa form |
PROTECTED WHEN COMPLETED - B
PAGE 1 OF 1
SPECIALIST'S REFERRAL FORM
Date |
|
UCI number: |
|
IME number: |
|
UMI number (if applicable): |
Attach image |
|
Family name: |
Gender: |
Given name:
Date of birth
Identity document seen? |
No |
|
Yes |
Document type: |
Passport |
|
Government issued photo ID |
|
|||||||
|
|
||||||
|
|
|
|
|
|
|
|
If you have any concerns that the individual presenting to you does not match the identification and photo of the individual above, please notify my office immediately.
Referred to (Specialist name / address):
Referred by (Panel Physician name / address):
Reason for referral:
Report to include:
•Clinical findings with current clinical status;
•Diagnosis;
•Pathology report if available;
•Treatment recommendations;
•Prognosis for the next five (5) years; and
•Copies of diagnostic tests and reports done as part of your investigations.
Specialist declaration:
I declare that I have examined the above client and the attached report is a true and correct record of my findings.
|
|
Signature |
|
|
Date |
|
|
Please return this form along with your report |
to the Panel Physician noted above. |
||
|
|
Thanking you in advance for your assistance. |
|||
IMM 5734 |
(DISPONIBLE EN FRANÇAIS - IMM 5734 F) |
||||