
You'll be able to complete Form Lg 196 Il instantly using our PDFinity® PDF editor. To make our tool better and less complicated to use, we constantly work on new features, bearing in mind suggestions from our users. All it takes is a couple of simple steps:
Step 1: First, open the editor by clicking the "Get Form Button" at the top of this site.
Step 2: This tool helps you work with almost all PDF files in various ways. Modify it by writing your own text, adjust what's originally in the file, and include a signature - all within a couple of mouse clicks!
This PDF requires particular info to be filled out, hence ensure you take whatever time to provide exactly what is asked:
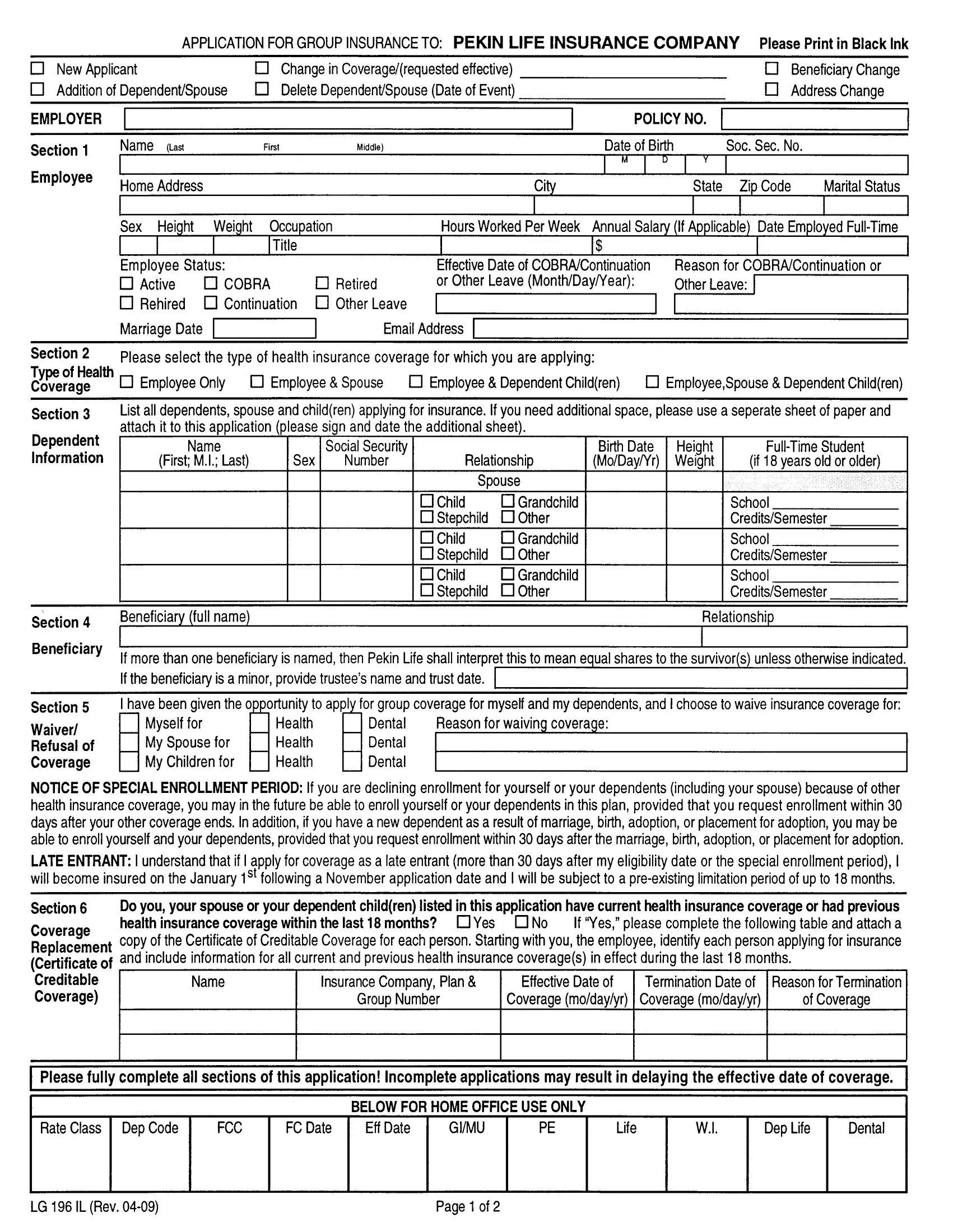
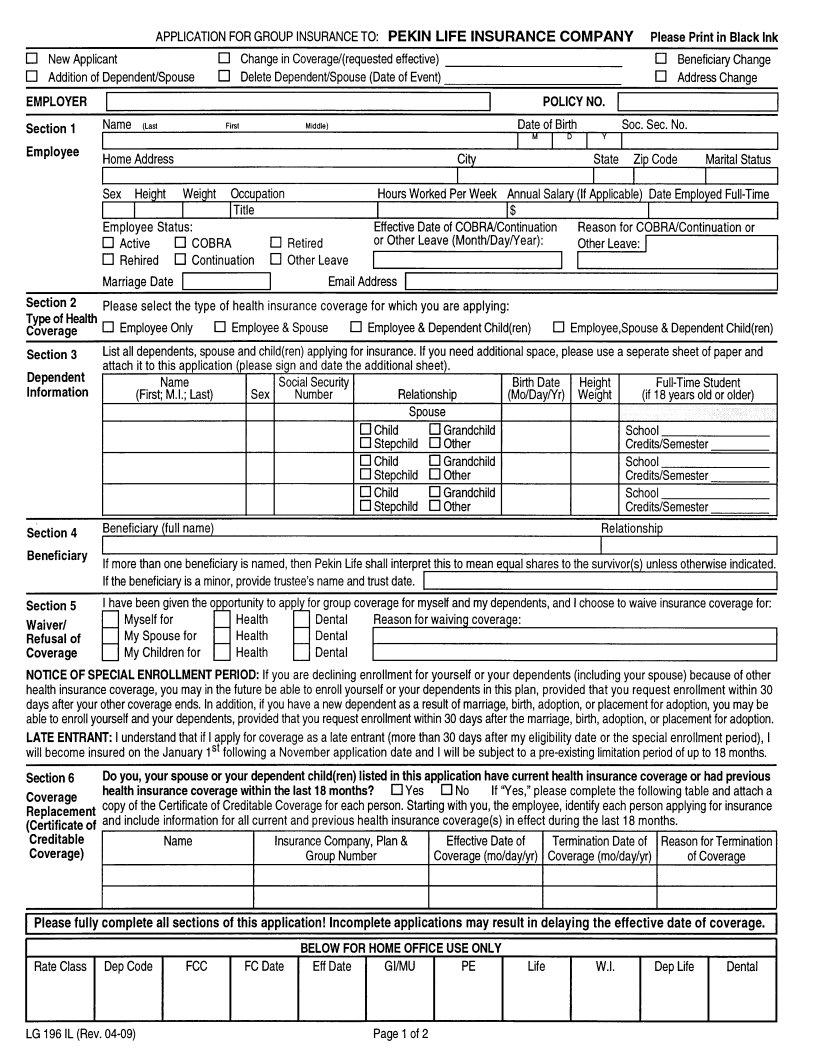
1. It's important to complete the Form Lg 196 Il properly, hence be attentive while filling out the sections containing these fields:
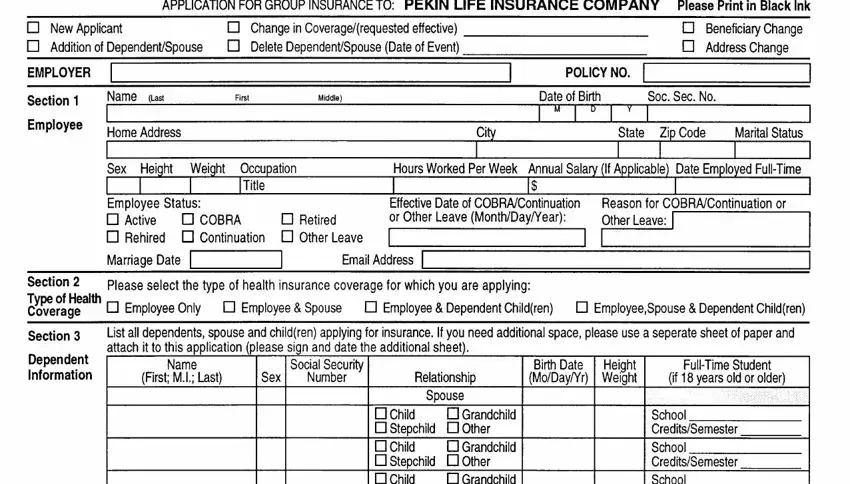
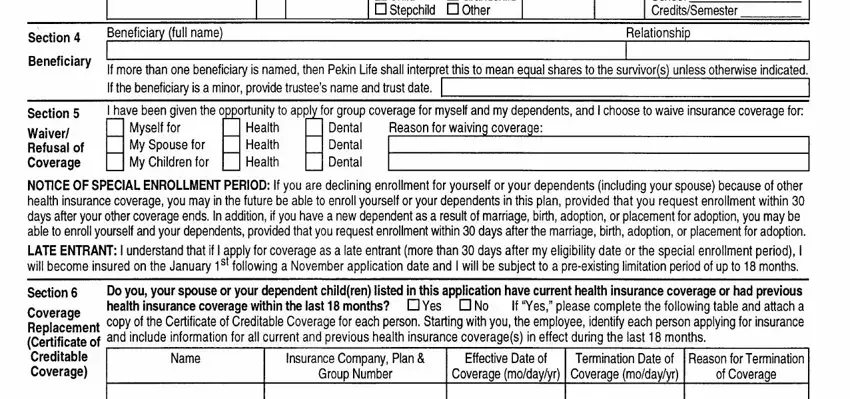
2. Now that this section is complete, you're ready include the needed details in n Child tr Stepchild I Other, Grandchild, Section, Beneficiary, lf more than one beneficiary lf, is a minor provide kustees name, is named, then Pekin Life shall interpret, this t mean equal, NOTICE OF SPECIAL ENROLLMENT PERID, including your spouse because of, that you request enrollment wrthin, tor yourself or your dependents, that if I apply for coverage as a, and for all current and previous so you're able to move forward to the next step.
3. Completing Please fully complete all sections, Incomplele applications may resull, Rate Class Dep Code, FCC, FC Date, Eff Date, GIMU, Life, Dep Life, Dental, BELOW FOR HOME OFFICE USE ONLY, LG lL Rev, and Page of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
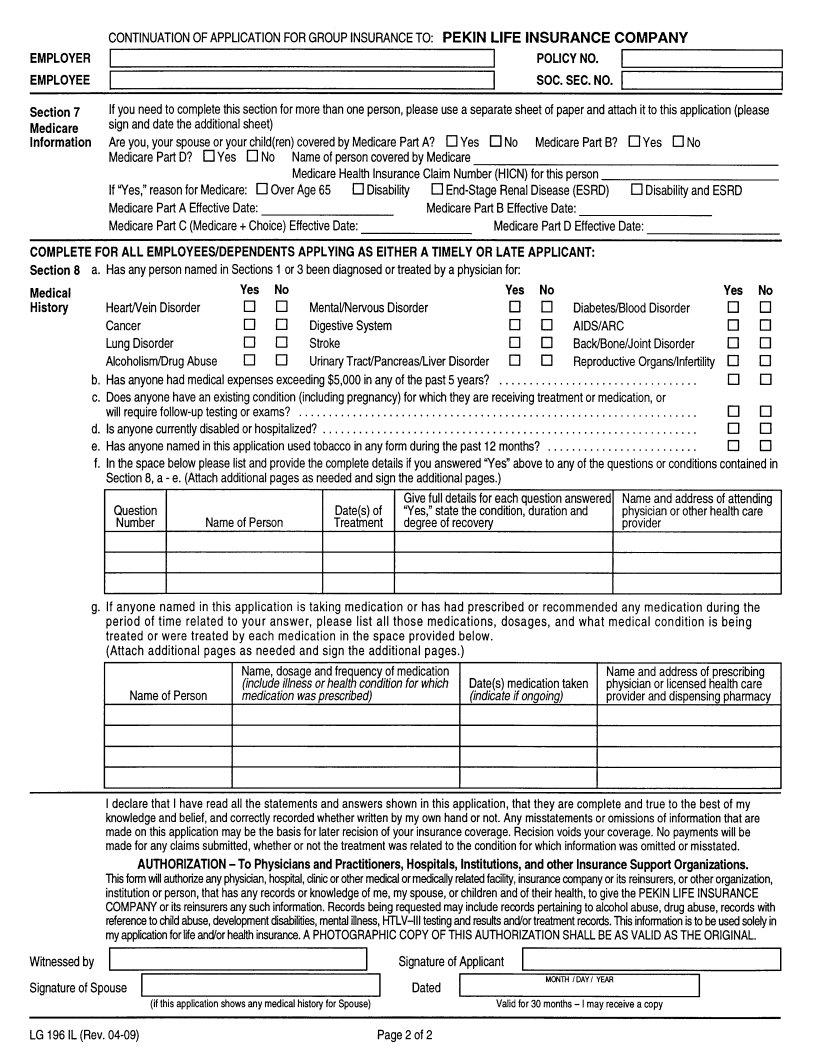
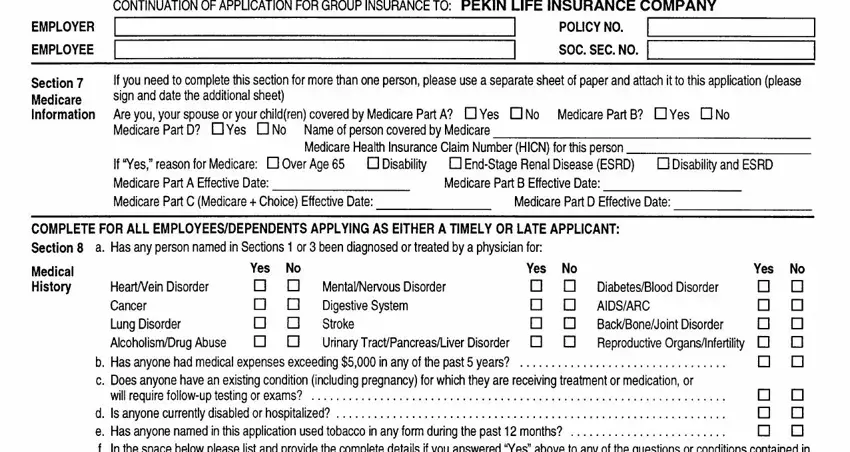
4. The next part requires your attention in the following areas: EMPLOYER, EMPLOYEE, Section Medicare lnformation, CONTINUATION, F APPLICATION FoR GROUP INSURANCE, POLICY NO soc sEc No, fiis section for more than one, please, lf you need to complete sign and, Yes nruo MedicarePartB, nYes ftrto, for Medicare, lf Yes reason Medicare Part A, flOver Age, and Medicare Part B Effective Date. Be sure that you fill in all of the required details to move further.
People generally make some mistakes when filling out CONTINUATION in this section. Remember to read twice what you type in right here.
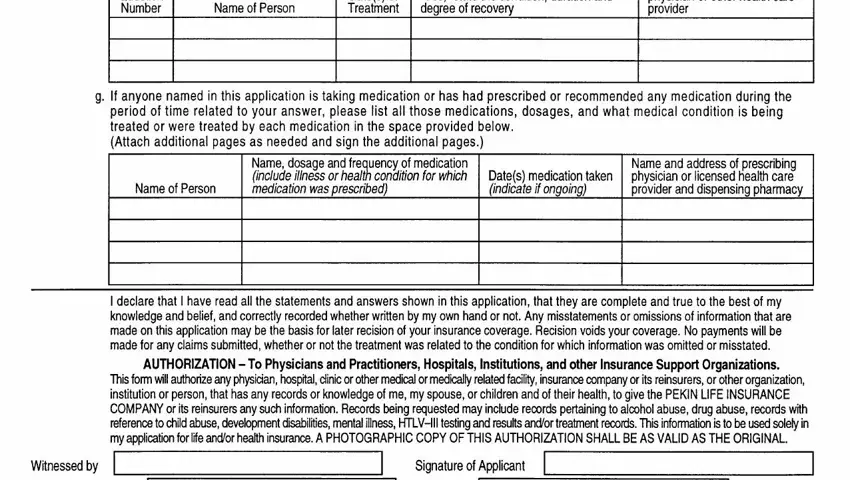
5. To finish your document, this last section requires some additional fields. Completing Question Number, Name of Person, Datesof Treatment, Give full details for each, Name and address of attendino, lf anyone named in this, is taking medication or has had, in the space provided below, any medication during the is being, Name of Person, Name dosaoe and freouencv of, Dates medication indicate if, taken, Name and address of orescribino, and liealth card will conclude the process and you'll certainly be done in a snap!
Step 3: Make sure the details are correct and then press "Done" to finish the process. Sign up with us right now and instantly get access to Form Lg 196 Il, all set for downloading. Every edit you make is conveniently saved , allowing you to change the document at a later stage when required. FormsPal guarantees your information privacy by using a protected method that in no way saves or distributes any sort of personal data involved. Be assured knowing your docs are kept safe whenever you use our services!