It's very easy to fill in the service community care empty blanks. Our PDF tool can make it almost effortless to fill out any specific form. Down the page are the only four steps you need to take:
Step 1: Step one will be to click on the orange "Get Form Now" button.
Step 2: So you should be on the document edit page. You can add, modify, highlight, check, cross, insert or erase areas or words.
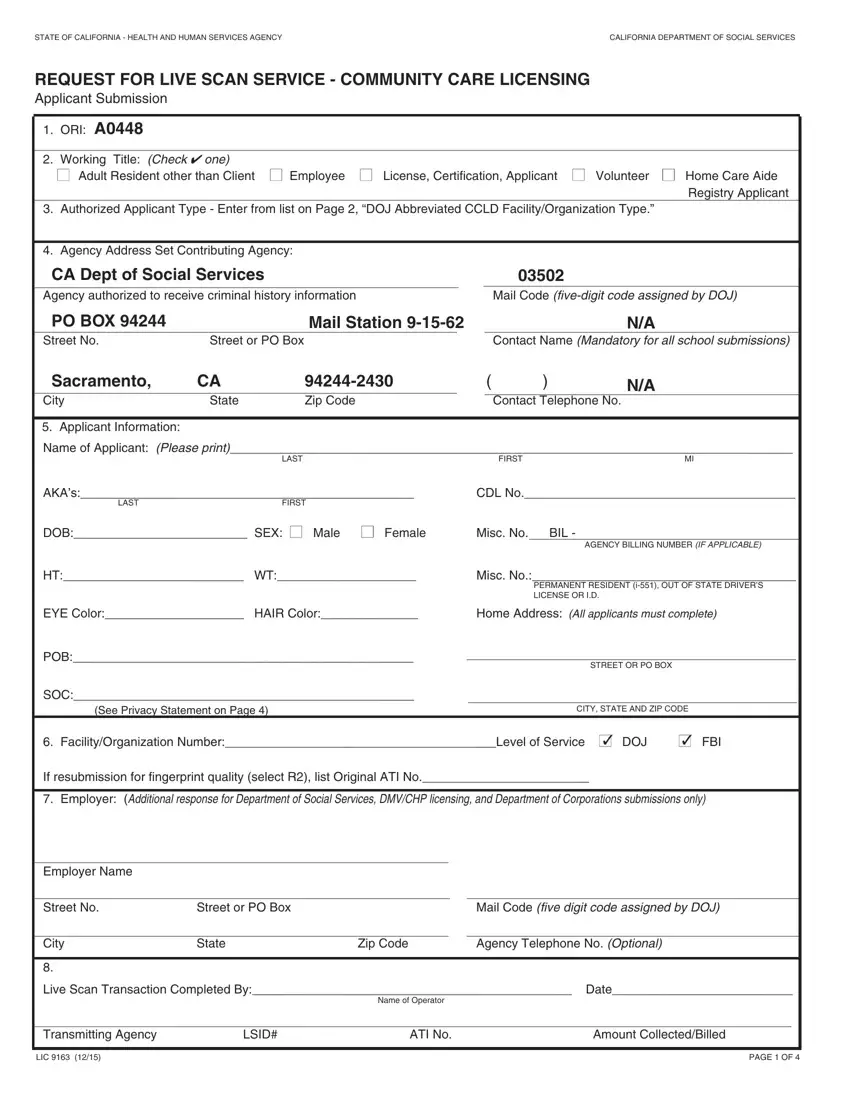
For each section, fill out the information required by the application.
Include the expected information in the HT WT, Misc No, PERMANENT RESIDENT i OUT OF STATE, EYE Color HAIR Color, Home Address All applicants must, POB, SOC, See Privacy Statement on Page, STREET OR PO BOX, CITY STATE AND ZIP CODE, FacilityOrganization NumberLevel, FBI, If resubmission for fingerprint, Employer Additional response for, and Employer Name box.
Step 3: The moment you select the Done button, the ready document is easily transferable to each of your devices. Or alternatively, it is possible to send it by means of mail.
Step 4: Make sure you remain away from forthcoming difficulties by creating no less than a pair of copies of your file.
