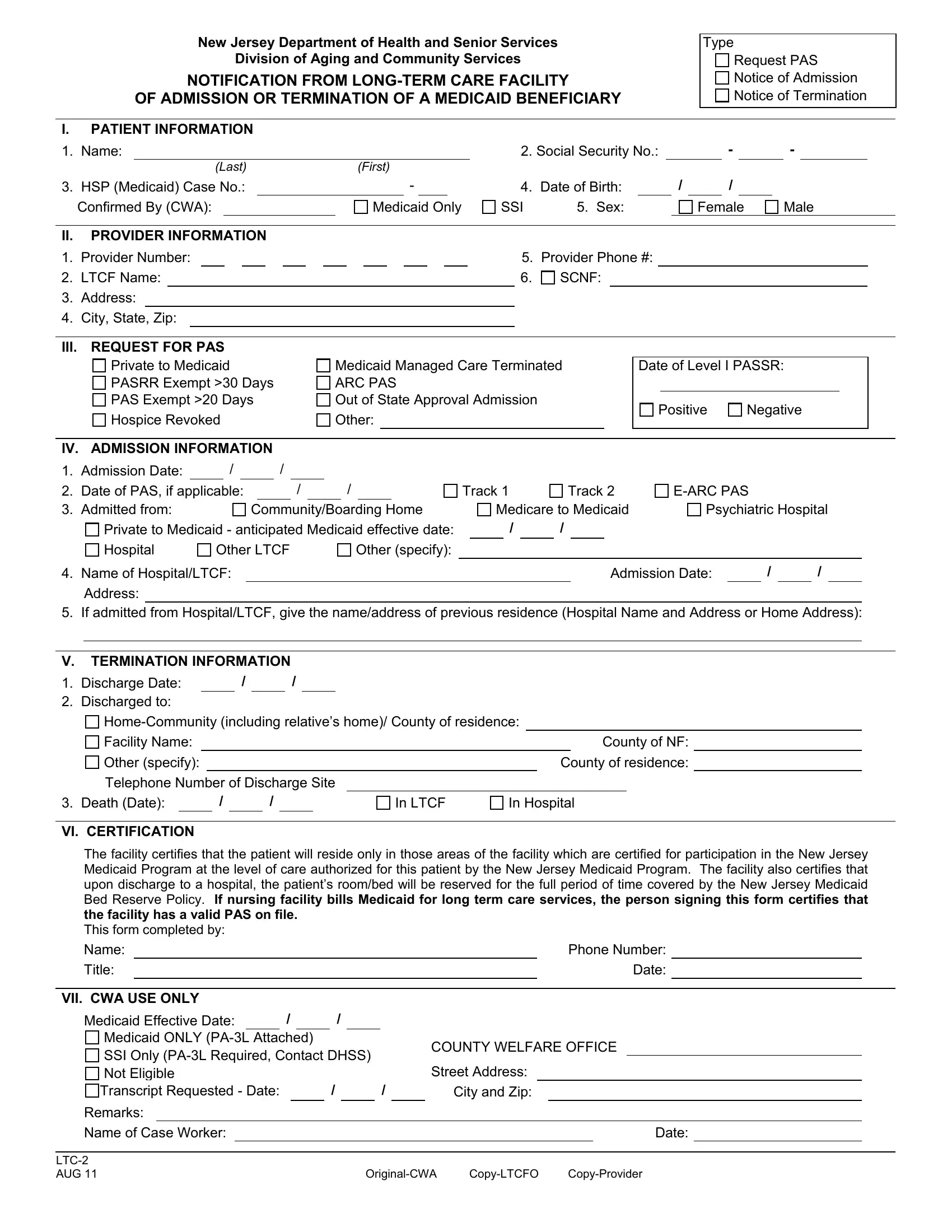
Navigating the complexities of long-term care for Medicaid beneficiaries in New Jersey involves important documentation, one piece of which is the LTC-2 form. This essential document, issued by the New Jersey Department of Health and Senior Services, Division of Aging and Community Services, serves multiple critical functions, primarily to notify about the admission or termination of a Medicaid beneficiary in a long-term care facility. It encompasses detailed sections including patient information, like the individual’s name, social security number, Medicaid case number, and date of birth, which are crucial for identification and proper handling of each case. Provider information is also captured to link the patient to the specific care facility involved. The form also addresses requests for Pre-Admission Screening and Resident Review (PASRR), which determines if Medicaid beneficiaries require long-term care services and what level of care is appropriate. Admission and termination information sections further document key dates and transitions for the beneficiary, ensuring a clear record of their care journey. Importantly, the certification by the care facility attests to the beneficiary’s eligibility for Medicaid-covered services and the facility’s compliance with relevant Medicaid policies. This form, vital for both the administration of Medicaid and the welfare of the beneficiaries, reflects a step in ensuring that long-term care facilities provide the necessary and appropriate care for their residents.
| Question | Answer |
|---|---|
| Form Name | Form Ltc 2 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CWA, pasrr level 2 nj, nj pasrr level ii determination letter sample, SSI |
New Jersey Department of Health and Senior Services |
Type |
Division of Aging and Community Services |
Request PAS |
NOTIFICATION FROM |
Notice of Admission |
OF ADMISSION OR TERMINATION OF A MEDICAID BENEFICIARY |
Notice of Termination |
I.PATIENT INFORMATION
1. |
Name: |
|
|
|
|
|
2. Social Security No.: |
|
|
- |
|
|
- |
|
|
|||||
|
|
(LAST) |
|
(FIRST) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
3. |
HSP (Medicaid) Case No.: |
|
- |
|
|
4. |
Date of Birth: |
|
|
/ |
|
/ |
|
|
|
|
|
|||
|
Confirmed By (CWA): |
|
|
Medicaid Only |
SSI |
5. Sex: |
|
|
Female |
Male |
|
|||||||||
II.PROVIDER INFORMATION
1. |
Provider Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Provider Phone #: |
|
|||
2. |
LTCF Name: |
|
|
6. |
SCNF: |
|
||||||||||||||
3.Address:
4.City, State, Zip:
III. REQUEST FOR PAS
Private to Medicaid PASRR Exempt >30 Days PAS Exempt >20 Days Hospice Revoked
Medicaid Managed Care Terminated
ARC PAS
Out of State Approval Admission
Other:
Date of Level I PASSR:
|
|
|
|
Positive |
Negative |
||
|
|
|
|
IV. |
ADMISSION INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
1. |
Admission Date: |
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
2. |
Date of PAS, if applicable: |
|
|
/ |
|
|
/ |
|
|
Track 1 |
|
Track 2 |
|
|
|
|
|||||||||||
3. |
Admitted from: |
|
|
|
Community/Boarding Home |
|
Medicare to Medicaid |
Psychiatric Hospital |
|||||||||||||||||||
|
Private to Medicaid - anticipated Medicaid effective date: |
/ |
/ |
|
|
|
|
|
|
|
|
||||||||||||||||
|
Hospital |
Other LTCF |
|
Other (specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
4. |
Name of Hospital/LTCF: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Admission Date: |
/ |
/ |
|
|||||||
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
If admitted from Hospital/LTCF, give the name/address of previous residence (Hospital Name and Address or Home Address): |
||||||||||||||||||||||||||
V.TERMINATION INFORMATION
1. |
Discharge Date: |
|
|
|
|
/ |
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
2. |
Discharged to: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
Facility Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County of NF: |
|
||
|
Other (specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County of residence: |
|
|||
|
Telephone Number of Discharge Site |
|
|
|
|
|
|
|
|||||||||||||
3. |
Death (Date): |
|
|
/ |
|
|
/ |
|
|
|
|
|
In LTCF |
In Hospital |
|||||||
VI. CERTIFICATION
The facility certifies that the patient will reside only in those areas of the facility which are certified for participation in the New Jersey Medicaid Program at the level of care authorized for this patient by the New Jersey Medicaid Program. The facility also certifies that upon discharge to a hospital, the patient’s room/bed will be reserved for the full period of time covered by the New Jersey Medicaid Bed Reserve Policy. If nursing facility bills Medicaid for long term care services, the person signing this form certifies that the facility has a valid PAS on file.
This form completed by:
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number: |
|
|
|||||||
Title: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date: |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VII. CWA USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Medicaid Effective Date: |
|
|
/ |
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Medicaid ONLY |
|
|
|
|
|
|
COUNTY WELFARE OFFICE |
|
|
||||||||||||||
SSI Only |
|
|
|
||||||||||||||||||||
|
|
Street Address: |
|
|
|||||||||||||||||||
Not Eligible |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Transcript Requested - Date: |
|
|
|
|
/ |
|
|
|
/ |
|
City and Zip: |
|
|||||||||||
Remarks: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Name of Case Worker: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date: |
|
|
|||||
|
|
|
|
AUG 11 |