This PDF editor makes it easy to fill in forms. There's no need to perform much to manage MassHealth Adult Disability Supplement forms. Just follow the next actions.
Step 1: You can press the orange "Get Form Now" button at the top of the page.
Step 2: Now you're on the form editing page. You may enhance and add text to the form, highlight specified content, cross or check certain words, insert images, put a signature on it, erase unneeded areas, or eliminate them altogether.
These particular areas are what you will need to prepare to get your ready PDF document.
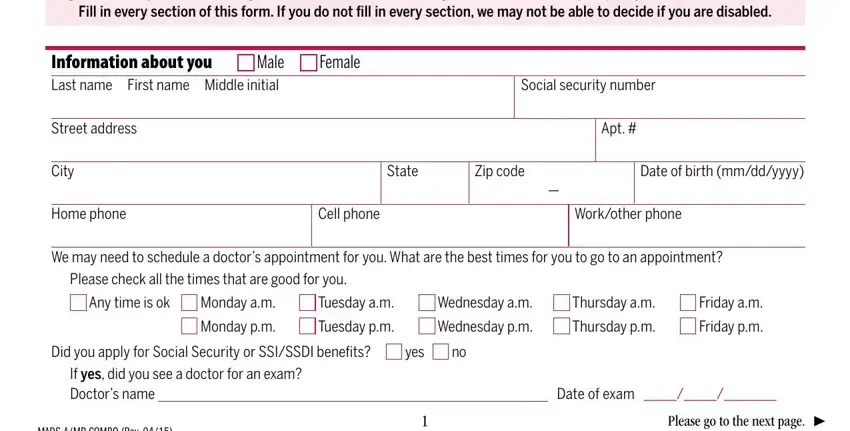
The software will require you to submit the If you need help with this form, Information about you Last name, Female, Male, Street address, Apt, City State Zip code Date of birth, Home phone Cell phone Workother, We may need to schedule a doctors, Please check all the times that, Any time is ok, Monday am, Tuesday am, Wednesday am, and Thursday am part.
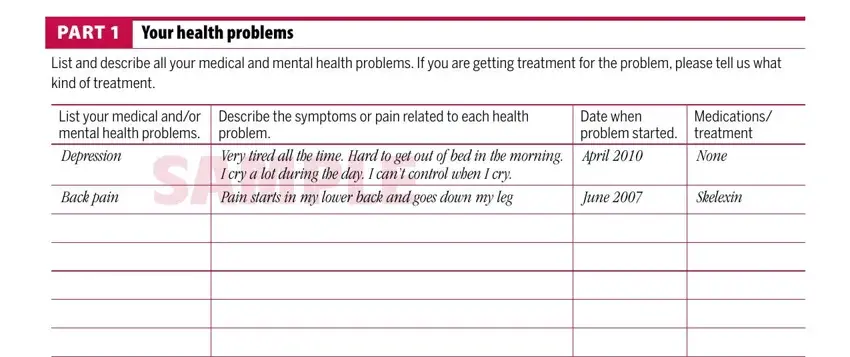
You could be required some relevant particulars to be able to prepare the PART Your health problems, List and describe all your medical, List your medical andor mental, Back pain, Describe the symptoms or pain, Date when problem started April, Medications treatment None, June, and Skelexin section.
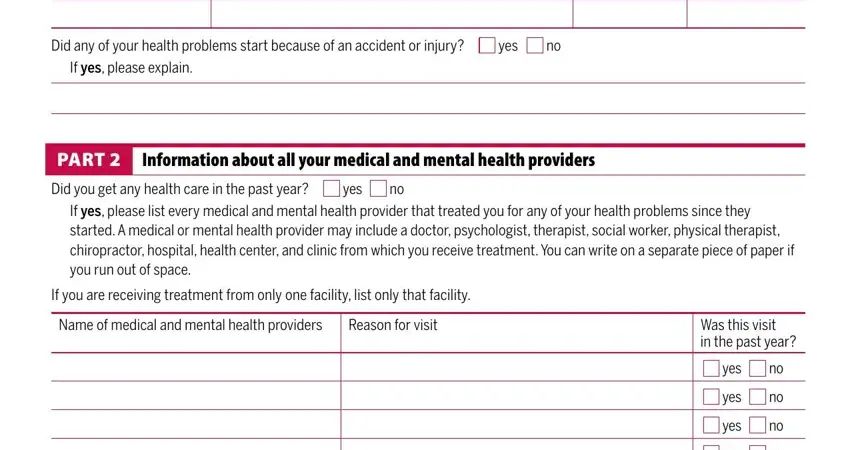
Within the section Did any of your health problems, yes, If yes please explain, PART Information about all your, Did you get any health care in the, yes, If yes please list every medical, If you are receiving treatment, Name of medical and mental health, Reason for visit, Was this visit in the past year, yes, yes, yes, and yes, write down the rights and obligations of the sides.
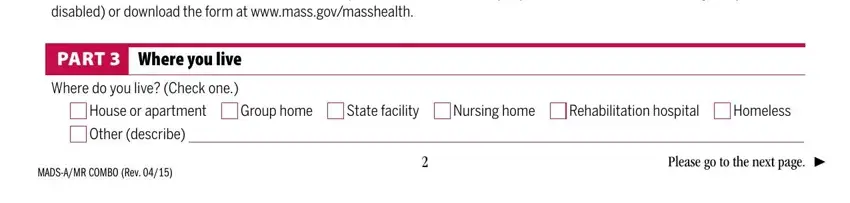
Fill in the file by checking the following fields: Please fill out a Medical Records, PART Where you live, Where do you live Check one, House or apartment, Group home, State facility, Nursing home, Rehabilitation hospital, Homeless, Other describe, MADSAMR COMBO Rev, and Please go to the next page.
Step 3: Hit the button "Done". Your PDF file can be exported. It's possible to upload it to your pc or send it by email.
Step 4: Make copies of the document. This may protect you from future challenges. We cannot watch or publish your data, thus feel comfortable knowing it will be protected.
