Our qualified developers have worked together to implement the PDF editor that you could apply. This specific software allows you to prepare Form Mdch Bcal 3305 documents immediately and conveniently. This is certainly all you should conduct.
Step 1: Hit the "Get Form Now" button to begin the process.
Step 2: At this point, you are on the document editing page. You may add content, edit present information, highlight certain words or phrases, place crosses or checks, add images, sign the template, erase unwanted fields, etc.
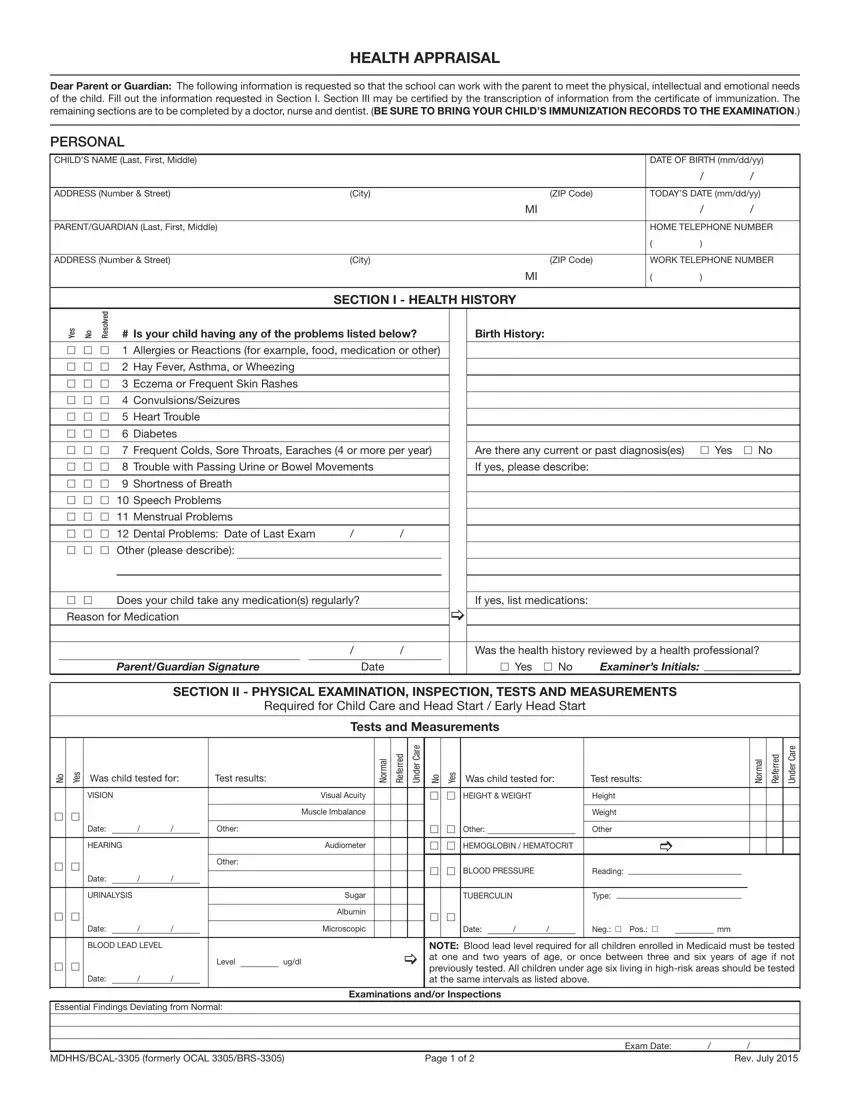
Prepare the Form Mdch Bcal 3305 PDF by typing in the content required for every single section.
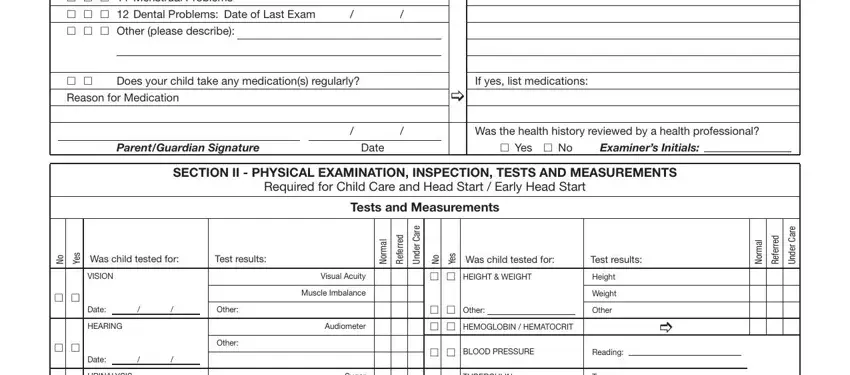
In the h h h Allergies or Reactions for, h h, Does your child take any, If yes list medications, Reason for Medication, ParentGuardian Signature, Date, Was the health history reviewed by, h Yes h No, Examiners Initials, SECTION II PHYSICAL EXAMINATION, Tests and Measurements, o N, s e Y, and Was child tested for area, put in writing your details.
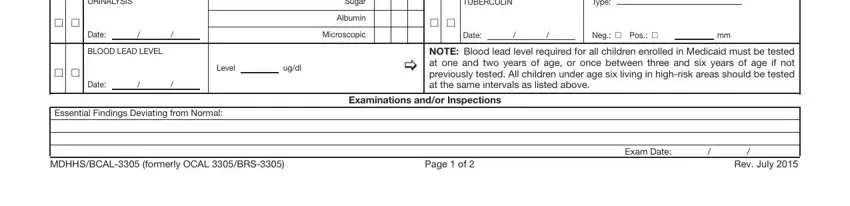
The application will require for more info as a way to effortlessly fill out the part URINALYSIS, h h, Date, BLOOD LEAD LEVEL, h h, Date, Type, TUBERCULIN, h h, Date, Neg h Pos h, NOTE Blood lead level required for, Sugar, Albumin, and Microscopic.
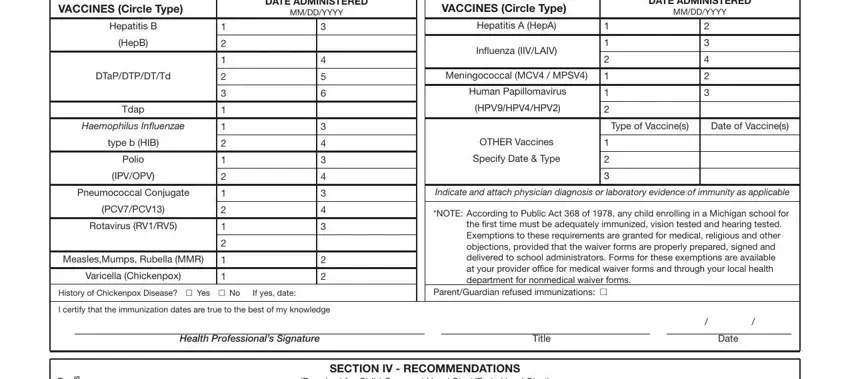
You need to define the rights and responsibilities of all parties in box VACCINES Circle Type, DATE ADMINISTERED MMDDYYYY, Hepatitis B, HepB, DTaPDTPDTTd, Tdap, Haemophilus Influenzae, type b HIB, Polio, IPVOPV, Pneumococcal Conjugate, PCVPCV, Rotavirus RVRV, MeaslesMumps Rubella MMR, and Varicella Chickenpox.
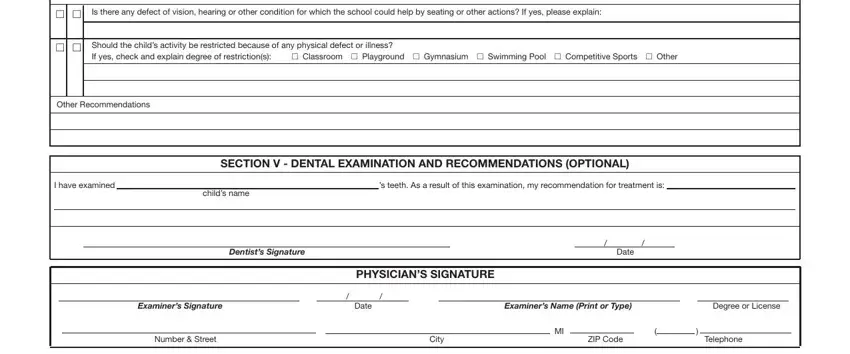
End by checking the following sections and filling them in as needed: Is there any defect of vision, Should the childs activity be, h Classroom h Playground h, h h, h h, Other Recommendations, I have examined, s teeth As a result of this, childs name, SECTION V DENTAL EXAMINATION AND, Dentists Signature, Date, PHYSICIANS SIGNATURE, Examiners Signature, and Date.
Step 3: The moment you hit the Done button, your ready document is conveniently exportable to any of your gadgets. Alternatively, you can send it via email.
Step 4: Generate a duplicate of each form. It will save you time and permit you to keep clear of challenges later on. Also, your information is not used or analyzed by us.
