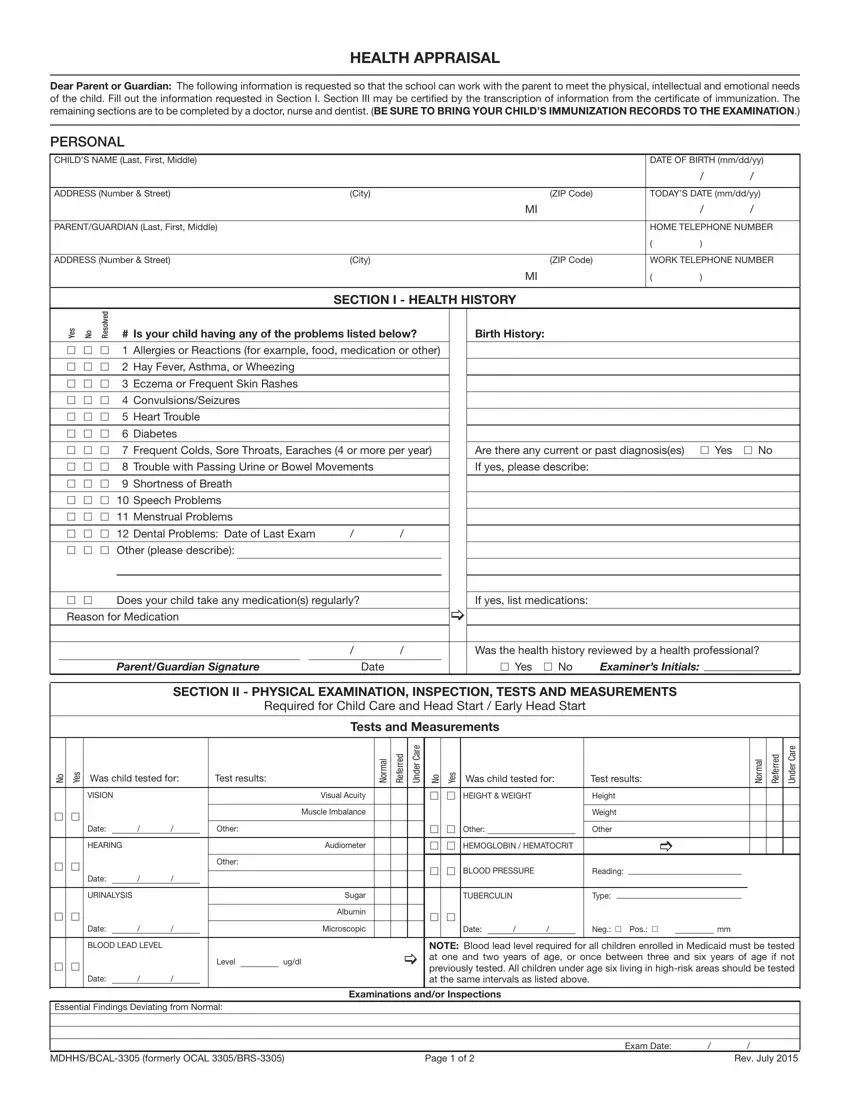
Ensuring the health and well-being of children as they embark on their educational journey is a pivotal aspect of collaborative care among parents, schools, and healthcare providers. The Mdch Bcal 3305 form, a comprehensive health appraisal document, serves as a cornerstone for this collaborative effort. It requests detailed information to assist schools in accommodating the physical, intellectual, and emotional needs of students. By requiring completion by parents or guardians, and certification by healthcare professionals, this form encompasses a child's health history, including allergies, chronic conditions, and medication needs, and specifies requirements for physical examinations, immunization records, and dental assessments. Crucially, the form facilitates the transcription of immunization information, underlining the importance of vaccination in school admission processes, while also addressing accommodations needed within the school environment to support the child's health and participation in various activities. Developed with input from an array of health and education stakeholders, the Mdch Bcal 3305 embodies a proactive approach to ensuring that children receive the necessary health checks, vaccinations, and care recommendations tailored to support their success in the educational setting.
| Question | Answer |
|---|---|
| Form Name | Form Mdch Bcal 3305 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Health Appraisal 1f18s4s webadvisor ohlone form |
