
polst form minnesota pdf can be completed online without difficulty. Just make use of FormsPal PDF editor to complete the task in a timely fashion. To make our tool better and simpler to work with, we continuously come up with new features, taking into account suggestions coming from our users. Here's what you'll want to do to begin:
Step 1: Firstly, access the tool by pressing the "Get Form Button" above on this site.
Step 2: After you launch the online editor, you'll notice the document ready to be completed. Besides filling in different fields, you may also perform other sorts of actions with the file, that is adding any words, editing the original text, adding images, placing your signature to the PDF, and more.
With regards to the blanks of this particular document, this is what you should do:
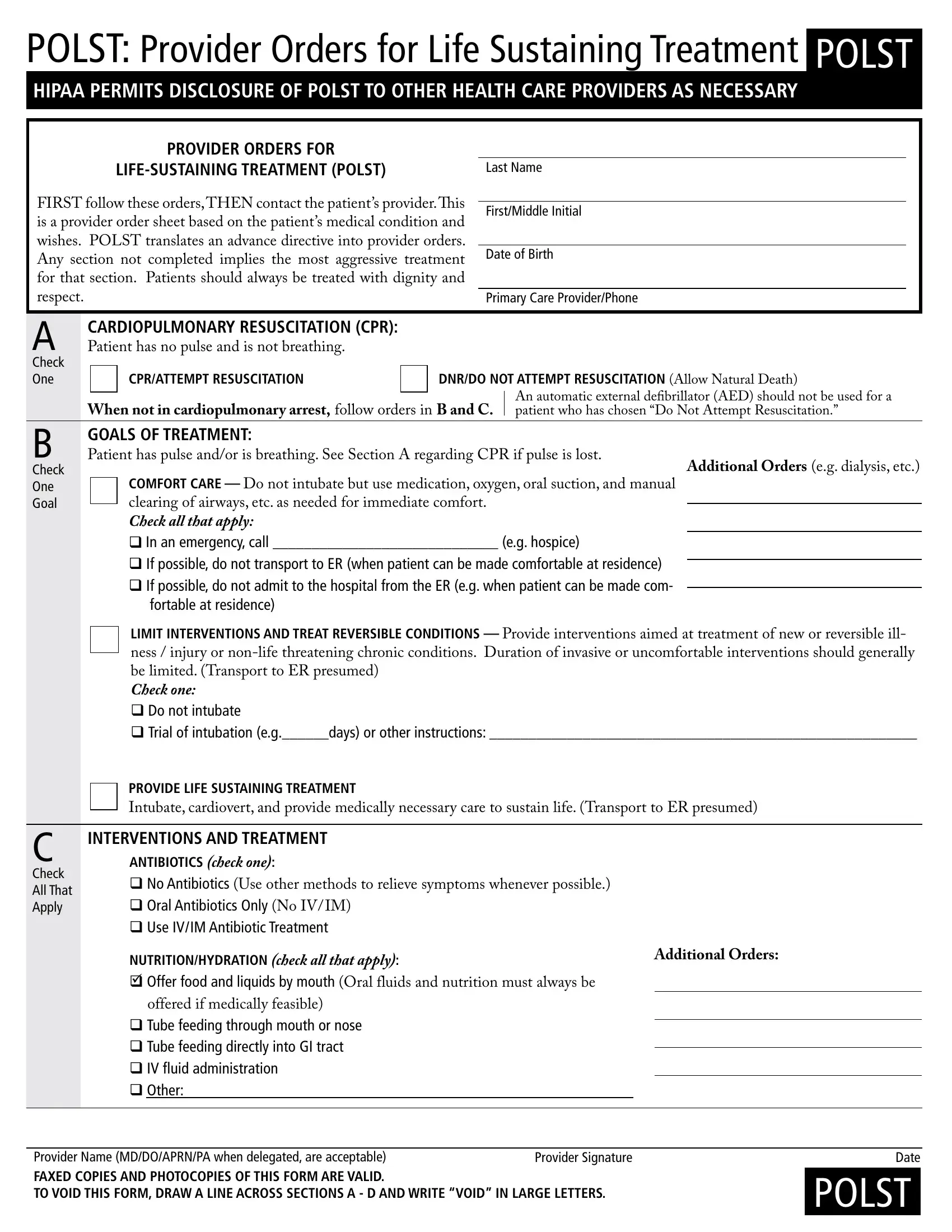
1. Fill out the polst form minnesota pdf with a selection of major fields. Get all the required information and be sure there's nothing left out!
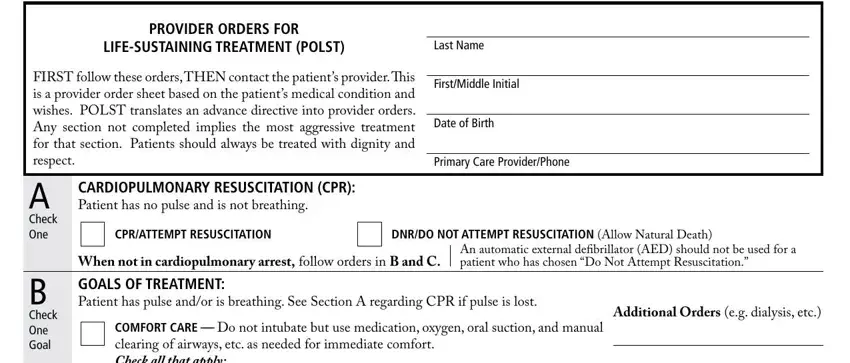
2. The next stage would be to submit the next few blank fields: COMFORT CARE Do not intubate but, In an emergency call eg hospice, fortable at residence, LIMIT INTERVENTIONS AND TREAT, PROVIDE LIFE SUSTAINING TREATMENT, Check All That Apply, INTERVENTIONS AND TREATMENT, and ANTIBIOTICS check one No.
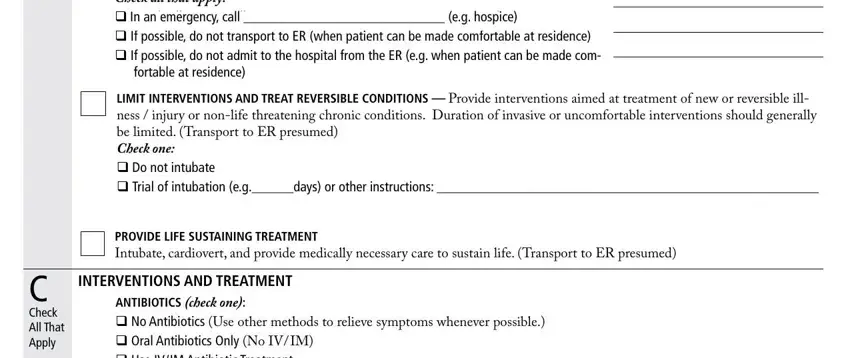
3. This stage is usually easy - fill in every one of the empty fields in NUTRITIONHYDRATION check all that, Additional Orders, offered if medically feasible, Tube feeding through mouth or, Provider Name MDDOAPRNPA when, Provider Signature, Date, and POLST to complete the current step.
In terms of Provider Name MDDOAPRNPA when and Date, ensure you get them right here. Both these could be the key fields in the file.
4. You're ready to fill out the next form section! Here you'll have all of these Check All That Apply, DISCUSSED WITH, PATIENT, PARENTS OF MINOR, HEALTH CARE AGENT, COURTAPPOINTED GUARDIAN, NONE, OTHER, POLST, THE BASIS FOR THESE ORDERS IS, REQUEST, BEST INTEREST, KNOWN PREFERENCE, OTHER, and HEALTH CARE DIRECTIVE LIVING WILL empty form fields to fill out.
Step 3: Spell-check the information you have typed into the blank fields and hit the "Done" button. Create a 7-day free trial subscription with us and get direct access to polst form minnesota pdf - with all changes saved and available from your FormsPal account. FormsPal provides risk-free form editing without personal data recording or sharing. Feel comfortable knowing that your data is safe with us!