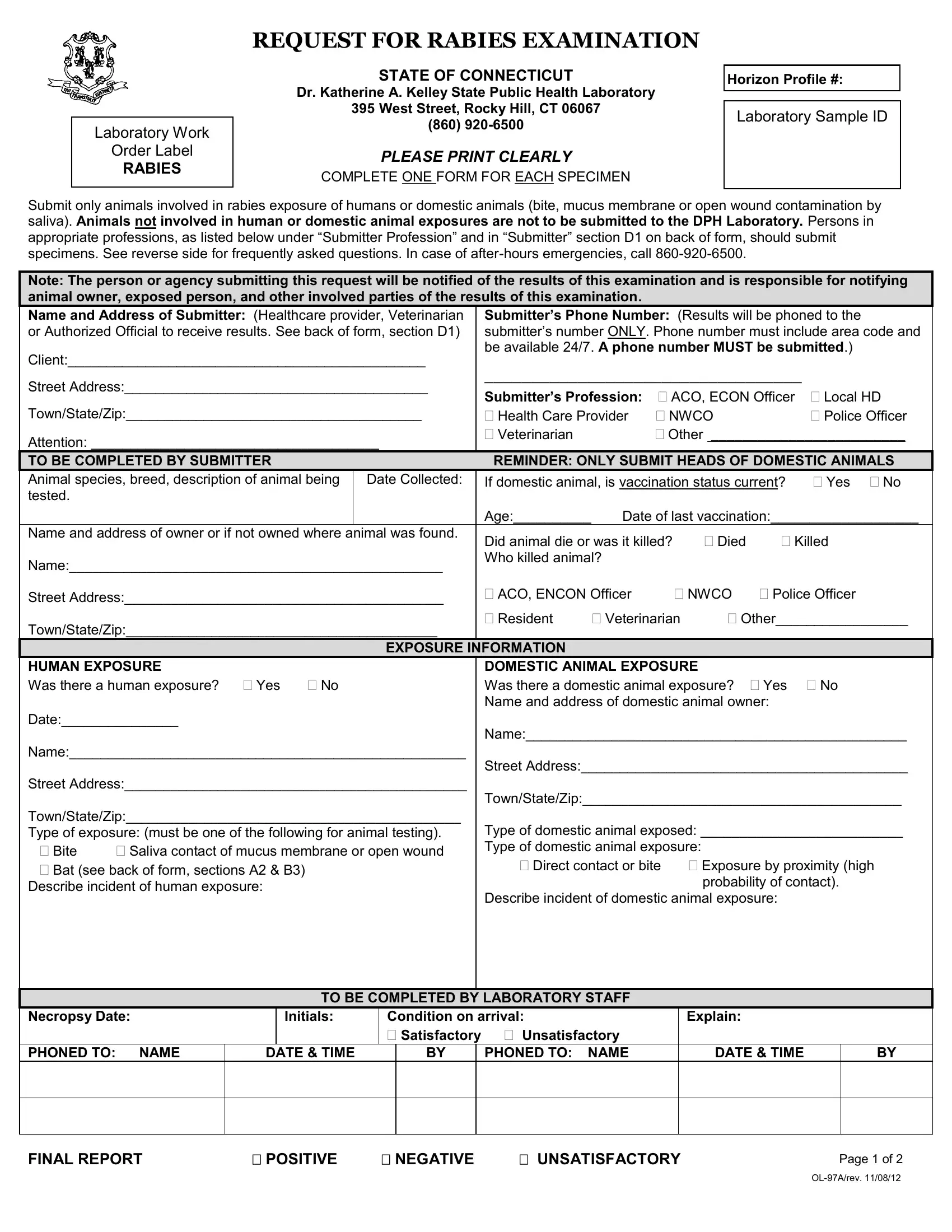
REQUEST FOR RABIES EXAMINATION
Laboratory Work
Order Label
RABIES
STATE OF CONNECTICUT
Dr. Katherine A. Kelley State Public Health Laboratory
395 West Street, Rocky Hill, CT 06067
(860) 920-6500
PLEASE PRINT CLEARLY
COMPLETE ONE FORM FOR EACH SPECIMEN
Horizon Profile #: ___
Laboratory Sample ID
Submit only animals involved in rabies exposure of humans or domestic animals (bite, mucus membrane or open wound contamination by
saliva). Animals not involved in human or domestic animal exposures are not to be submitted to the DPH Laboratory. Persons in appropriate professions, as listed below under “Submitter Profession” and in “Submitter” section D1 on back of form, should submit
specimens. See reverse side for frequently asked questions. In case of after-hours emergencies, call 860-920-6500.
Note: The person or agency submitting this request will be notified of the results of this examination and is responsible for notifying animal owner, exposed person, and other involved parties of the results of this examination.
|
Name and Address of Submitter: (Healthcare provider, Veterinarian |
Submitter’s Phone Number: (Results will be phoned to the |
|
|
or Authorized Official to receive results. See back of form, section D1) |
submitter’s number ONLY. Phone number must include area code and |
|
|
Client:______________________________________________ |
be available 24/7. A phone number MUST be submitted.) |
|
|
|
|
|
|
|
|
|
|
|
|
Street Address:_______________________________________ |
Submitter’s Profession: |
ACO, ECON Officer |
Local HD |
|
|
|
|
|
|
|
|
Town/State/Zip:______________________________________ |
Health Care Provider |
NWCO |
|
Police Officer |
|
|
Attention: _____________________________________ |
Veterinarian |
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE COMPLETED BY SUBMITTER |
|
|
REMINDER: ONLY SUBMIT HEADS OF DOMESTIC ANIMALS |
|
|
Animal species, breed, description of animal being |
Date Collected: |
If domestic animal, is vaccination status current? |
Yes No |
|
|
tested. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Age:__________ |
Date of last vaccination:___________________ |
|
|
Name and address of owner or if not owned where animal was found. |
Did animal die or was it killed? |
Died |
Killed |
|
|
|
|
|
|
|
|
Name:________________________________________________ |
Who killed animal? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address:_________________________________________ |
ACO, ENCON Officer |
NWCO |
Police Officer |
|
|
|
|
|
|
|
|
|
|
|
|
Town/State/Zip:________________________________________ |
Resident |
Veterinarian |
|
Other_________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXPOSURE INFORMATION |
|
|
|
|
|
|
|
|
|
HUMAN EXPOSURE |
|
|
DOMESTIC ANIMAL EXPOSURE |
|
|
|
|
|
Was there a human exposure? Yes |
No |
Was there a domestic animal exposure? |
Yes |
No |
|
|
|
|
|
|
Name and address of domestic animal owner: |
|
|
|
|
Date:_______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name:_________________________________________________ |
|
|
Name:___________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address:__________________________________________ |
|
|
Street Address:____________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Town/State/Zip:_________________________________________ |
|
|
Town/State/Zip:___________________________________________ |
|
|
|
|
|
|
|
|
|
|
Type of exposure: (must be one of the following for animal testing). |
Type of domestic animal exposed: __________________________ |
|
|
Bite |
Saliva contact of mucus membrane or open wound |
Type of domestic animal exposure: |
|
|
|
|
|
Bat (see back of form, sections A2 & B3) |
|
|
Direct contact or bite |
Exposure by proximity (high |
|
|
|
|
|
|
|
probability of contact). |
|
|
Describe incident of human exposure: |
|
|
|
|
|
|
|
|
|
Describe incident of domestic animal exposure: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE COMPLETED BY LABORATORY STAFF |
|
|
|
|
|
|
|
Necropsy Date:
PHONED TO: NAME
|
Initials: |
Condition on arrival: |
Explain: |
|
|
|
Satisfactory |
Unsatisfactory |
|
|
DATE & TIME |
|
BY |
|
PHONED TO: NAME |
DATE & TIME |
BY |
|
|
|
|
|
|
|
|
FINAL REPORT |
POSITIVE |
NEGATIVE |
UNSATISFACTORY |
Page 1 of 2 |
|
|
|
|
OL-97A/rev. 11/08/12 |
INSTRUCTIONS FOR SUBMITTING SPECIMENS FOR RABIES TESTING
Animals are tested to guide medical management of humans or domestic animals who have interactions with suspect rabid animals. The DPH and local health departments are available to assist persons exposed and responders who may evaluate potential exposures to determine the need for animal testing.
A. Types of animals accepted for rabies examination:
1.Raccoons, skunks, wild carnivores (e.g., fox, coyote, bobcat) and groundhogs that have bitten a person or domestic animal.
2.Bats that have direct contact or are found in a room with a person who cannot communicate seeing it or knowing they may have been bitten (e.g., sleeping person, baby or young child, person with dementia, or someone inebriated).
3.Wild animals must be killed without damaging the head and submitted immediately for examination.
B.Submit for testing ONLY after consultation with the DPH or local health department:
1.Animals that have not bitten a person or domestic animal.
2.Small rodents (e.g., mice, rats, squirrels, chipmunks, moles) and rabbits that have bitten a person or domestic animal. These animals are rarely found to be rabid and rabies in these animals has not been detected in Connecticut.
3.Bats found in a home but not in a room with a person.
C.Submit for testing ONLY if instructed to by an Animal Control Officer:
1.Cats, dogs, and other domestic animals that have bitten a person or domestic animal.
∙These animals should usually be observed in quarantine for 14 days.
∙Contact the Department of Agriculture, Animal Control Division for questions concerning quarantine of domestic animals, (860) 713-2506
NEVER submit live animals. Domestic animals submitted whole must weigh less than 10 lbs. Submit only the head of domestic animals weighing more than 10 pounds. Arrangements for testing of livestock should be made with UCONN.
D.SUBMITTER
1.The authorized person who will be notified of the results and will provide consultation regarding the need for testing the animal (ACO, Environmental Conservation Police (ENCON) Officer, healthcare provider, local HD, NWCO, police officer, veterinarian, other ____________).
2.Local health department will be notified of results from animals submitted by unauthorized submitters.
PROPER SPECIMEN PACKAGING
Double-bag the specimen in leak-proof plastic bags. Place double-bag with specimen on ice in a leak proof container. Deliver specimen(s) to the laboratory as soon as possible.
IMPORTANT: Only ONE specimen per double-bag. Secure paperwork to the outside of the double-bag. Secure second set (copy) of paperwork on the outside of the leak proof container.
LABORATORY HOURS
The Virology Laboratory is staffed Monday - Friday from 7:30 a.m. - 4:00 p.m. Please bring specimens to the Katherine A. Kelley State Public Health Laboratory located at 395 West Street in Rocky Hill. Due to enhanced security, identification will be needed to proceed to the building. Once through the first gate, follow signs to Sample Receiving and Deliveries. At the second gate, press the buzzer and security will allow entrance. Proceed to the first turn-off on the right and park. Walk to the loading dock and press the buzzer for admittance to the building. Specimens should be brought to the Receiving Room down the corridor on the right side, where staff will take custody of the specimen. After hours, security will escort you to a walk-in cooler where the specimen and paperwork can be left. In case of after-hours emergencies, call 860-920-6500.
REQUISITION FORM
A completed request form must accompany each individual specimen submitted for testing. Please print clearly. The submitter’s phone number must be included for notification of results. Place the completed request form in an envelope and
secure it to the outside of each individual double-bagged specimen being submitted for testing.
ADDITIONAL INFORMATION
∙For questions concerning human exposure and prophylaxis, as well as to discuss the possibility of submitting animals uncommon to rabies infection, contact the Connecticut Department of Public Health, Epidemiology and Emerging Infections Program at (860) 509-7994 or your local health department.
∙For questions concerning livestock and domestic animal exposures (e.g., biting, quarantine, vaccination), contact the Department of Agriculture, Animal Control Division or the State Veterinarian at (860) 713-2506.
∙For questions regarding submission of livestock for testing (e.g., cost, requirements) contact the UCONN Veterinary Medical Diagnostic Laboratory at (860) 486-3738.
∙For questions concerning wildlife (unusual behavior, rabies, exposures to, etc.) contact the Department of Energy & Environmental Protection, Wildlife Division at (860) 424-3011. For emergencies call (860) 424-3333.
∙For additional information or for reporting incidents of animals biting people or domestic animals, please contact your local Animal Control Officer.
Page 2 of 2
OL-97A/rev. 11/08/12