
Northumberland can be filled out online effortlessly. Simply use FormsPal PDF tool to do the job fast. The tool is constantly updated by our staff, receiving handy functions and turning out to be greater. To get the ball rolling, consider these simple steps:
Step 1: First of all, open the pdf editor by clicking the "Get Form Button" at the top of this webpage.
Step 2: With the help of our online PDF tool, it is easy to do more than just fill out blank form fields. Edit away and make your docs look faultless with custom textual content added, or tweak the original content to excellence - all supported by an ability to insert any kind of graphics and sign the file off.
It's straightforward to fill out the form using out detailed tutorial! Here's what you have to do:
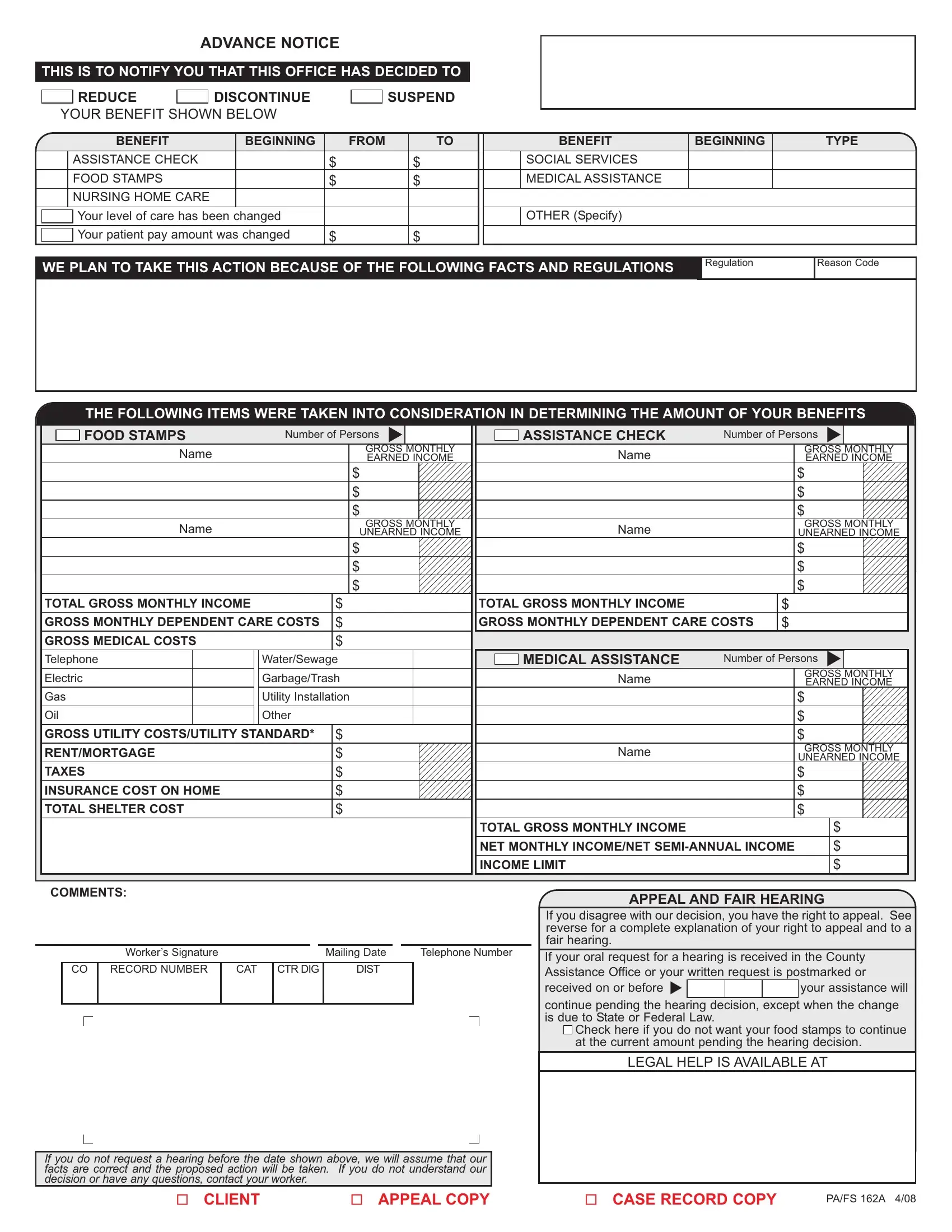
1. First, once completing the Northumberland, start in the page containing next blanks:
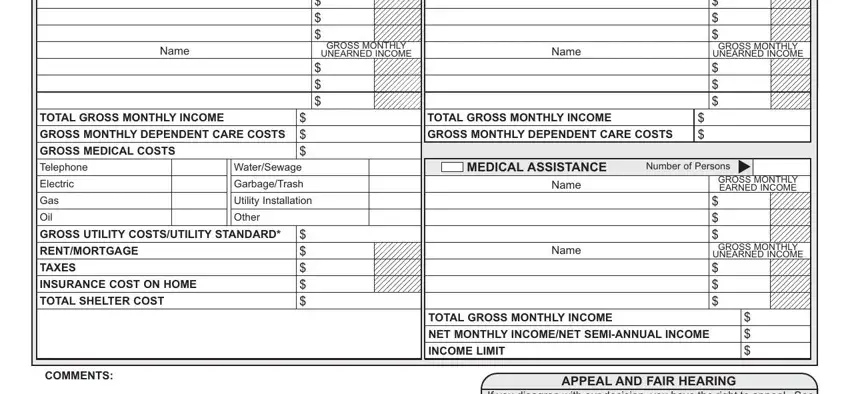
2. After the first part is completed, go to type in the applicable information in these: Name, GROSS MONTHLY, UNEARNED INCOME, Name, GROSS MONTHLY, UNEARNED INCOME, TOTAL GROSS MONTHLY INCOME, GROSS MONTHLY DEPENDENT CARE COSTS, GROSS MEDICAL COSTS, Telephone, Electric, Gas, Oil, WaterSewage, and GarbageTrash.
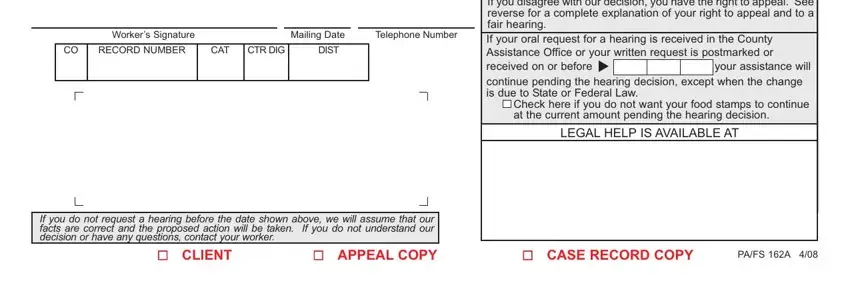
3. Completing Workers Signature, Mailing Date, Telephone Number, RECORD NUMBER, CAT, CTR DIG, DIST, If you disagree with our decision, cid, Check here if you do not want your, LEGAL HELP IS AVAILABLE AT, If you do not request a hearing, CLIENT APPEAL COPY, CASE RECORD COPY, and PAFS A is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
People who use this PDF frequently make some mistakes while filling in CLIENT APPEAL COPY in this section. You need to reread what you type in here.
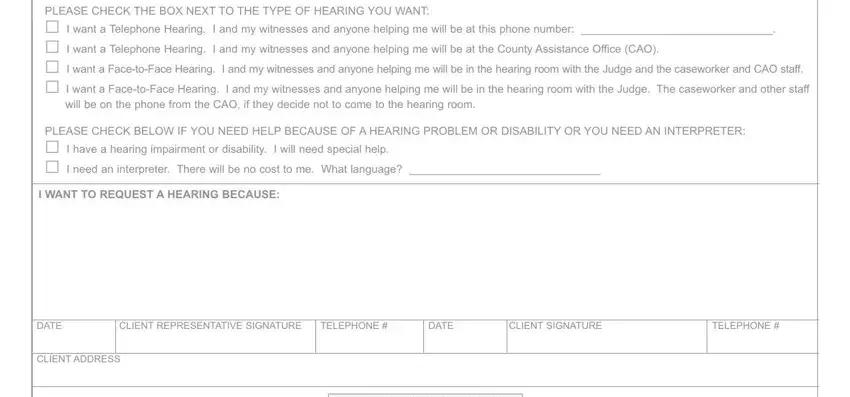
4. You're ready to complete this next form section! Here you've got all of these PLEASE CHECK THE BOX NEXT TO THE, will be on the phone from the CAO, PLEASE CHECK BELOW IF YOU NEED, I WANT TO REQUEST A HEARING BECAUSE, DATE, CLIENT REPRESENTATIVE SIGNATURE, TELEPHONE, DATE, CLIENT SIGNATURE, TELEPHONE, and CLIENT ADDRESS fields to fill out.
Step 3: Prior to obtaining the next step, check that all blanks have been filled in correctly. As soon as you think it's all fine, click on “Done." Sign up with us now and easily use Northumberland, prepared for download. All changes you make are preserved , enabling you to change the document at a later point as needed. If you use FormsPal, it is simple to complete documents without worrying about information incidents or records being distributed. Our protected software helps to ensure that your personal information is maintained safe.