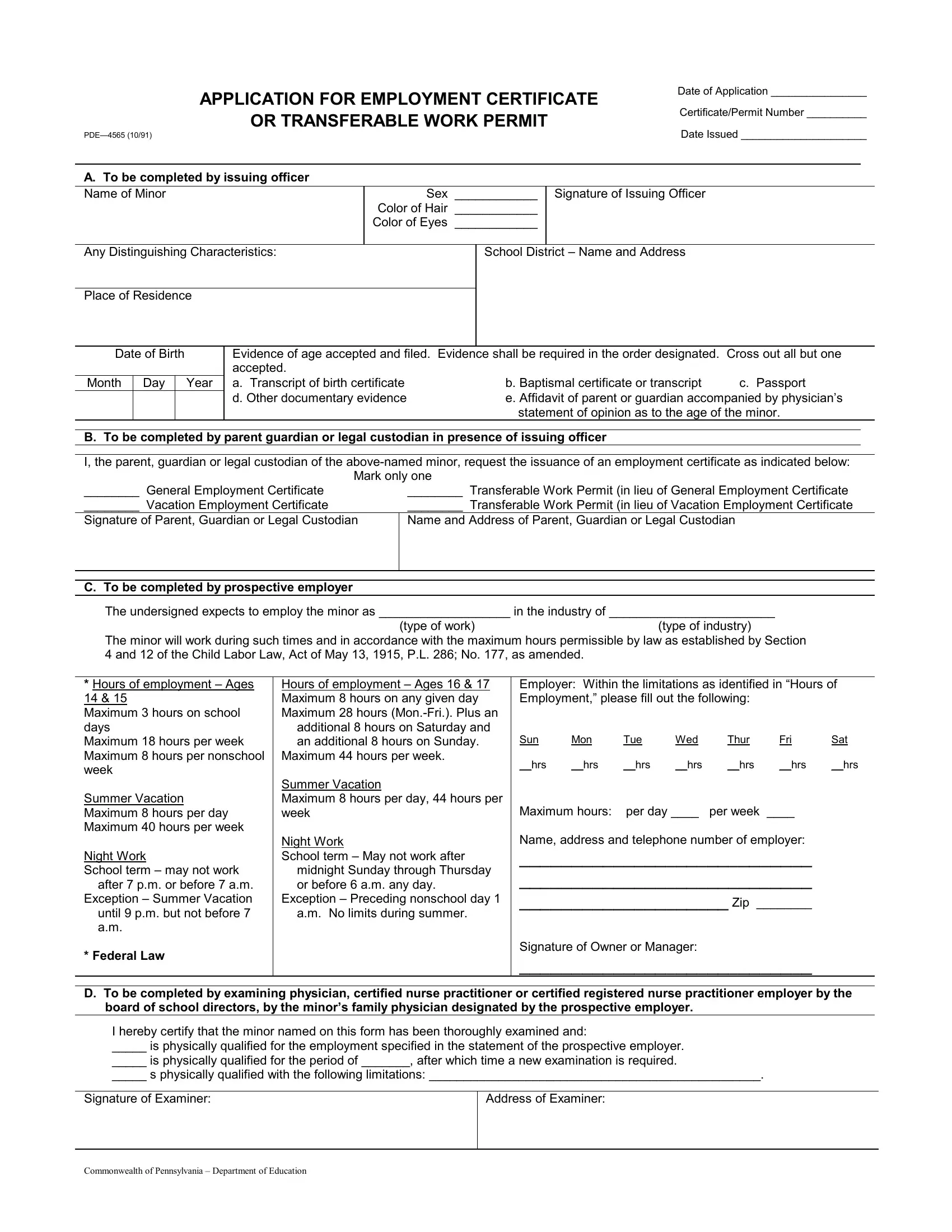
In navigating the complexities of employing minors, the PDE-4565 form serves as a cornerstone document, ensuring compliance with both state and federal regulations concerning child labor. This application for employment certificate or transferable work permit, delineated by the Commonwealth of Pennsylvania's Department of Education, stands as a pivotal step in the employment process of minors, offering a structured format for documenting essential information. It collects data starting from basic identifiers related to the minor—such as name, sex, physical characteristics, and residency—to more intricate details that include the type of employment certificate requested, parent or guardian consent, prospective employment details, and the hours of employment permissible under the law. Moreover, the form incorporates a section designated for a physician, certified nurse practitioner, or certified registered nurse practitioner to document health qualifications of the minor for the specified employment, in accordance with health standards laid out by the board of school directors or the minor’s own family physician endorsed by the prospective employer. This form not only encapsulates a procedure for lawful employment of minors but also underscores the importance of safeguarding their health and educational commitments, evidenced through its endorsements of age verification, informed parental or guardian consent, and medical fitness, structured within the legislative framework of the Child Labor Law, Act of May 13, 1915, as amended.
| Question | Answer |
|---|---|
| Form Name | Form PDE-4565 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 21 |
| Avg. time to fill out | 4 min 31 sec |
| Other names | form pde 4565 10 91, application for employment certificate, undersigned, TRANSFERABLE |