
Dealing with PDF documents online is always very simple using our PDF editor. You can fill out ssdi forms for doctors here without trouble. Our professional team is relentlessly endeavoring to develop the tool and ensure it is even better for people with its many features. Take full advantage of present-day innovative opportunities, and discover a myriad of unique experiences! All it requires is a couple of easy steps:
Step 1: Just click on the "Get Form Button" at the top of this site to start up our pdf file editing tool. There you will find everything that is needed to fill out your document.
Step 2: With the help of this state-of-the-art PDF editing tool, you'll be able to accomplish more than simply fill in forms. Try all the functions and make your forms look perfect with customized textual content incorporated, or optimize the original input to perfection - all that comes with an ability to add stunning images and sign the file off.
Pay close attention while filling out this pdf. Make certain every blank field is filled in correctly.
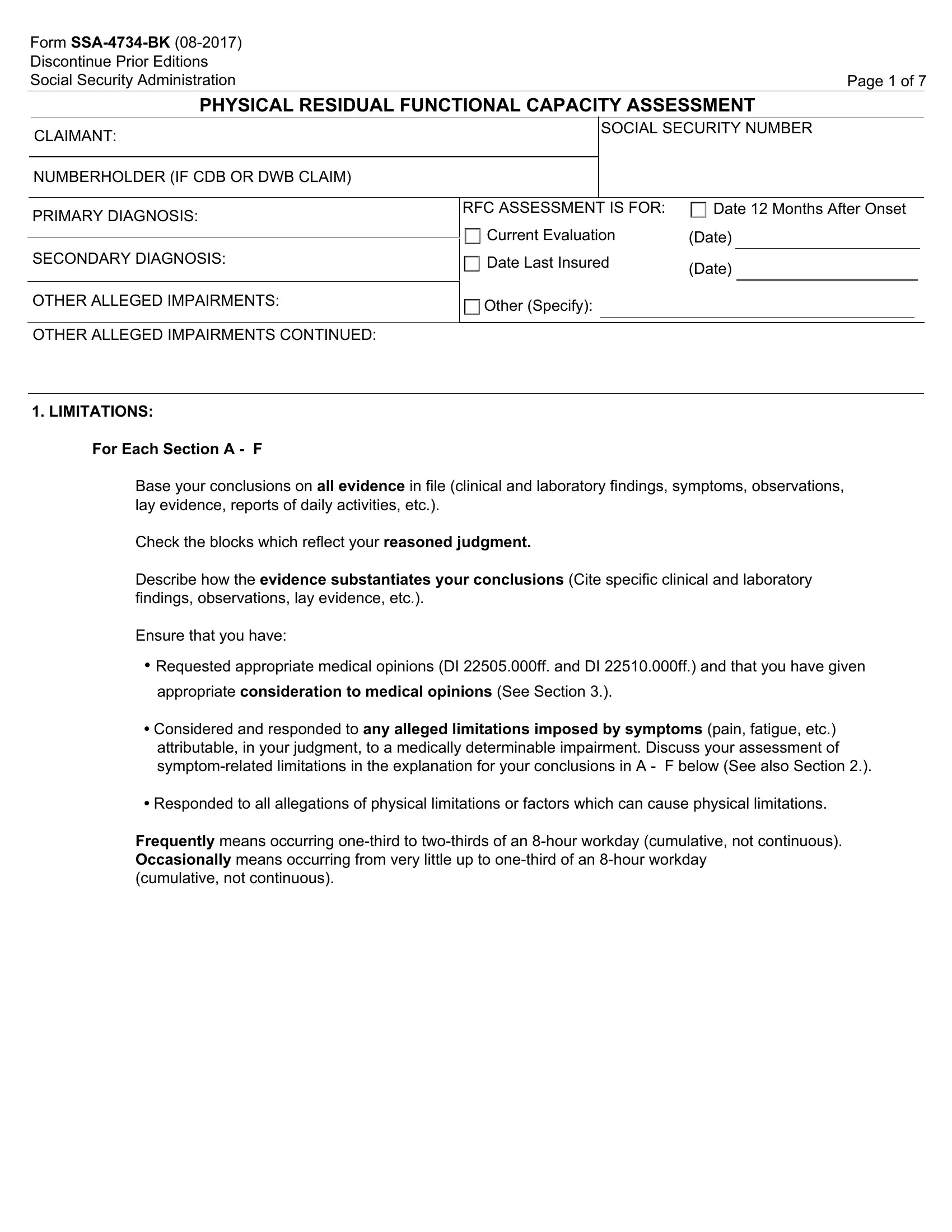
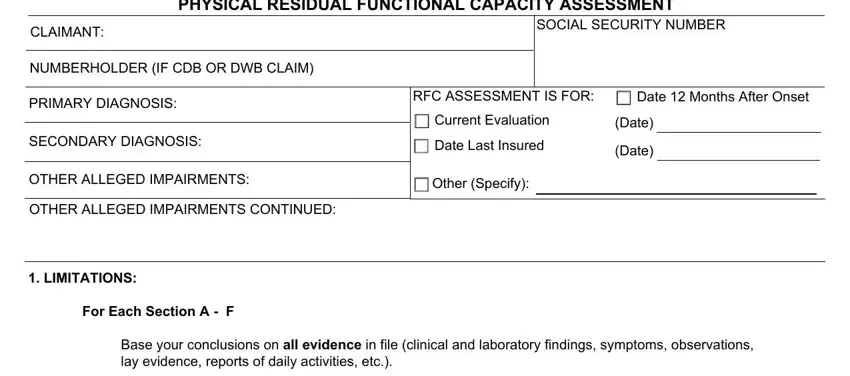
1. Fill out the ssdi forms for doctors with a number of essential blanks. Gather all the necessary information and make sure not a single thing overlooked!
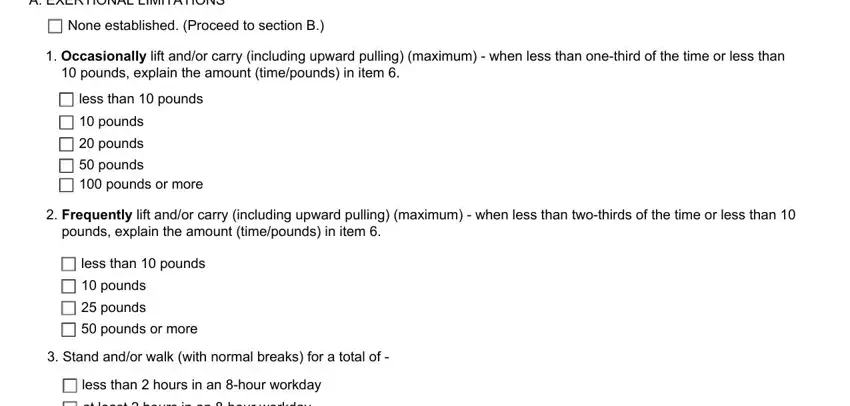
2. Once your current task is complete, take the next step – fill out all of these fields - A EXERTIONAL LIMITATIONS, None established Proceed to, Occasionally lift andor carry, less than pounds, pounds, pounds, pounds pounds or more, Frequently lift andor carry, less than pounds, pounds, pounds, pounds or more, Stand andor walk with normal, less than hours in an hour workday, and at least hours in an hour workday with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
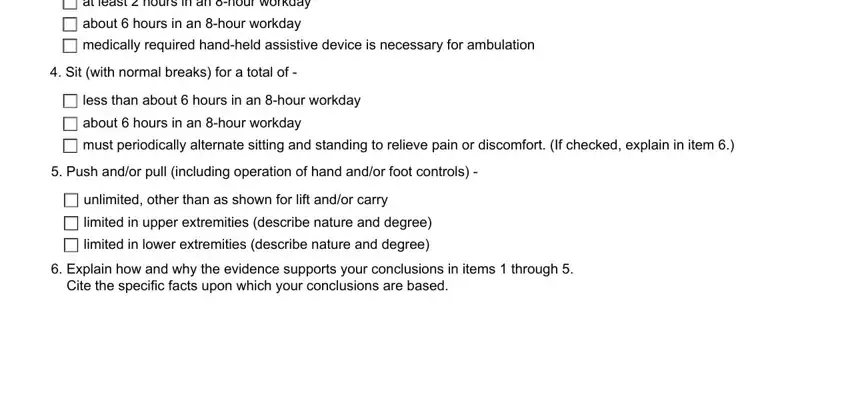
3. The following section is mostly about at least hours in an hour workday, about hours in an hour workday, medically required handheld, Sit with normal breaks for a, less than about hours in an hour, about hours in an hour workday, must periodically alternate, Push andor pull including, unlimited other than as shown for, limited in upper extremities, limited in lower extremities, and Explain how and why the evidence - complete each one of these empty form fields.
4. To move onward, this next stage will require filling out a few fields. These comprise of Frequently, Occasionally, Never, B POSTURAL LIMITATIONS, None established Proceed to, Climbing rampstairs, ladderropescaffolds, Balancing, Stooping, Kneeling, Crouching, Crawling, and When less than twothirds of the, which you'll find key to continuing with this particular form.
People who work with this PDF generally make errors while filling out When less than twothirds of the in this part. Make sure you reread everything you type in right here.
5. Since you draw near to the last parts of your form, there are a few extra requirements that need to be fulfilled. Mainly, C MANIPULATIVE LIMITATIONS, None established Proceed to, Reaching all directions including, Handling gross manipulation, Fingering fine manipulation, Feeling skin receptors, LIMITED, UNLIMITED, and Describe how the activities must be done.
Step 3: Ensure the details are accurate and then just click "Done" to complete the project. Sign up with FormsPal today and easily gain access to ssdi forms for doctors, all set for download. Every single edit made is conveniently kept , so that you can edit the form at a later point if necessary. When using FormsPal, you can easily complete forms without worrying about data breaches or entries being shared. Our protected software makes sure that your private data is maintained safe.