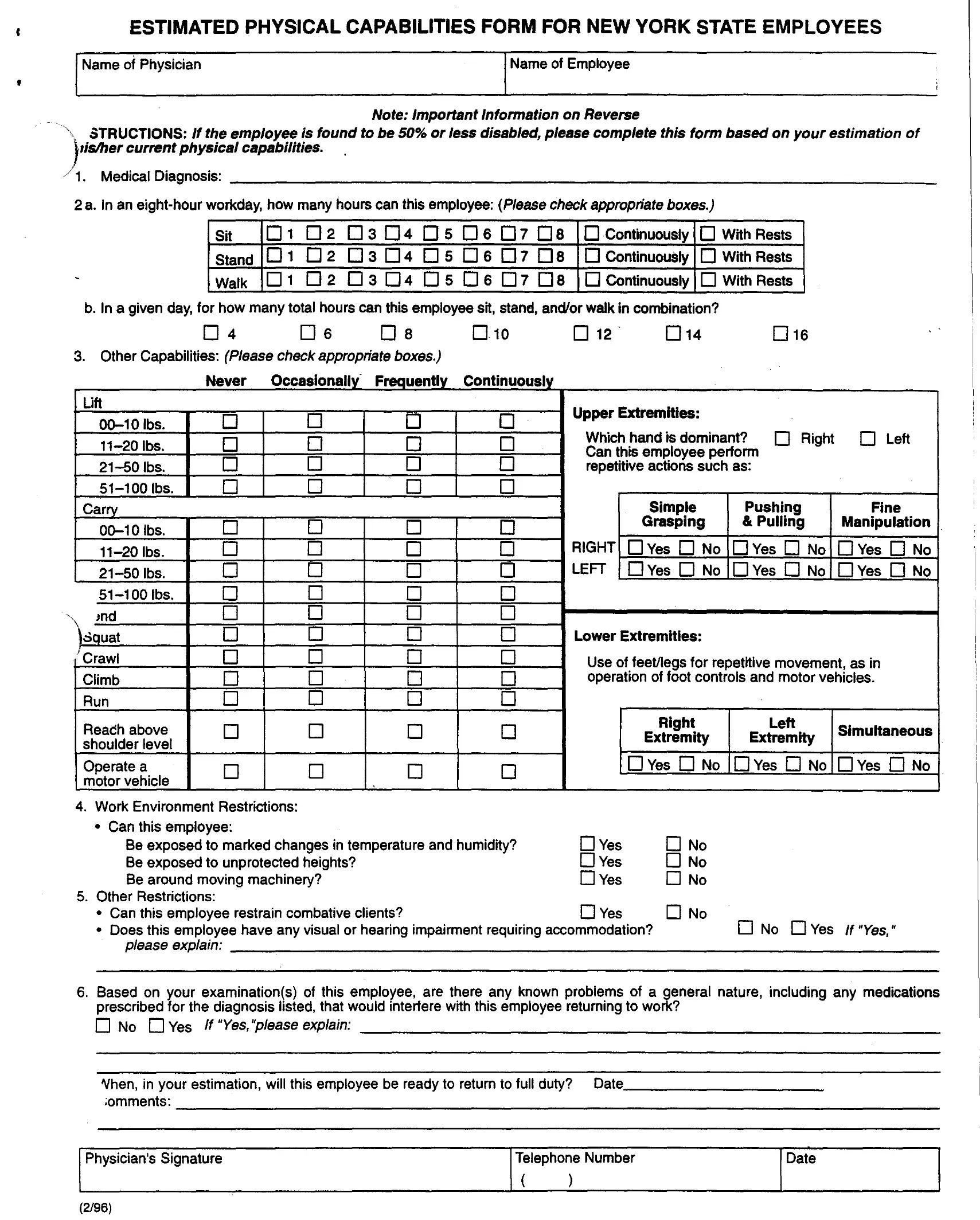
The Physical Capabilities form serves as a critical tool for assessing an employee’s ability to perform work-related tasks following an injury or illness. Completed by a physician, it offers a comprehensive evaluation of an employee's capacity by addressing various physical demands, including the ability to sit, stand, walk, lift, carry, push, and pull, along with the endurance to perform these activities over an eight-hour workday. Not only does it inquire about the employee's ability to perform repetitive actions with their upper and lower extremities, but it also delves into their capacity to engage in activities that require fine manipulation and the operation of motor vehicles. Additionally, the form evaluates potential work environment restrictions, such as exposure to extreme temperatures, humidity, and moving machinery, as well as other specific restrictions like dealing with combative clients or working at unprotected heights. Furthermore, it assesses any visual or hearing impairments that might necessitate special accommodations. Physicians are also asked to note any general health issues exacerbated by prescribed medications or treatments that could impede the employee’s return to work, providing a space for them to estimate when the individual might be able to resume full duty. This careful documentation is essential for employers to make informed decisions regarding workplace accommodations and the safety and well-being of their employees.
| Question | Answer |
|---|---|
| Form Name | Physical Capabilities Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | physical capability form, ny estimated capabilities, ny physical capabilities state form, ny estimated physical state pdf |