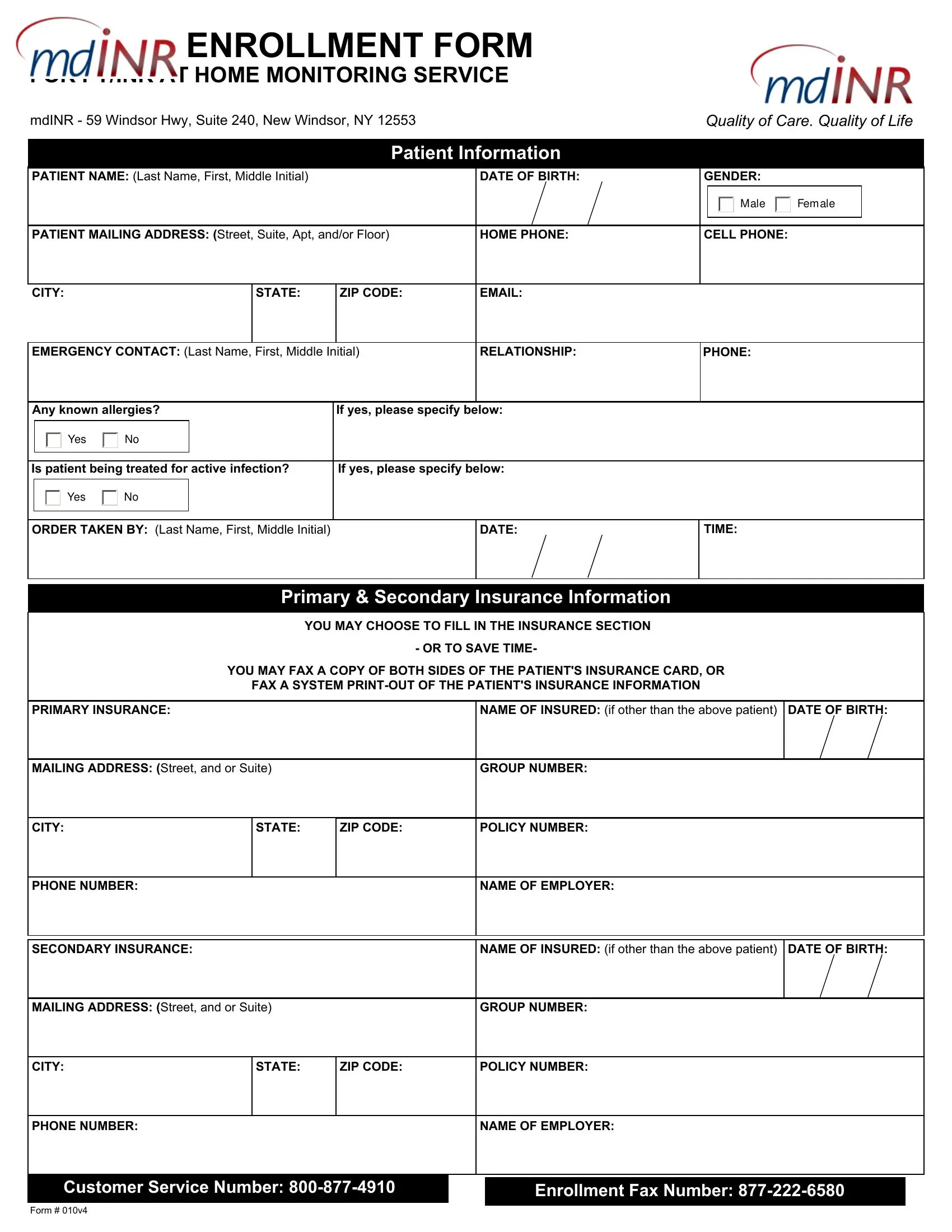
Navigating the complexities of healthcare, the PT/INR form emerges as a crucial tool for patients requiring anticoagulation therapy, facilitating their enrollment in home monitoring services. Located at 59 Windsor Hwy, Suite 240, New Windsor, NY, mdINR emphasizes the enhancement of both care quality and life quality through this form. The document gathers comprehensive patient information, including name, address, allergies, and the presence of any active infections, underscoring the personalized approach to each patient's care. Moreover, it details insurance information meticulously, allowing for a streamlined process in securing coverage for the service. The form extends to capture the prescribing physician's details, reinforcing the collaborative care model between the patient, healthcare providers, and mdINR. A significant section is dedicated to the Statement of Medical Necessity and Prescription, which underscores the critical nature of regular INR tests for patients on warfarin therapy, to prevent the risks associated with irregular blood coagulation levels. It specifies the patient’s diagnosis, setting forth a care plan that includes the target INR range and test frequency, ensuring precise monitoring. This document not only represents an administrative requirement but also a gateway to safer, more efficient patient care in the landscape of anticoagulation management.
| Question | Answer |
|---|---|
| Form Name | Form Pt Inr |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form inr pdf, mdinr enrollment form, form enrollment inr, mdinr form |