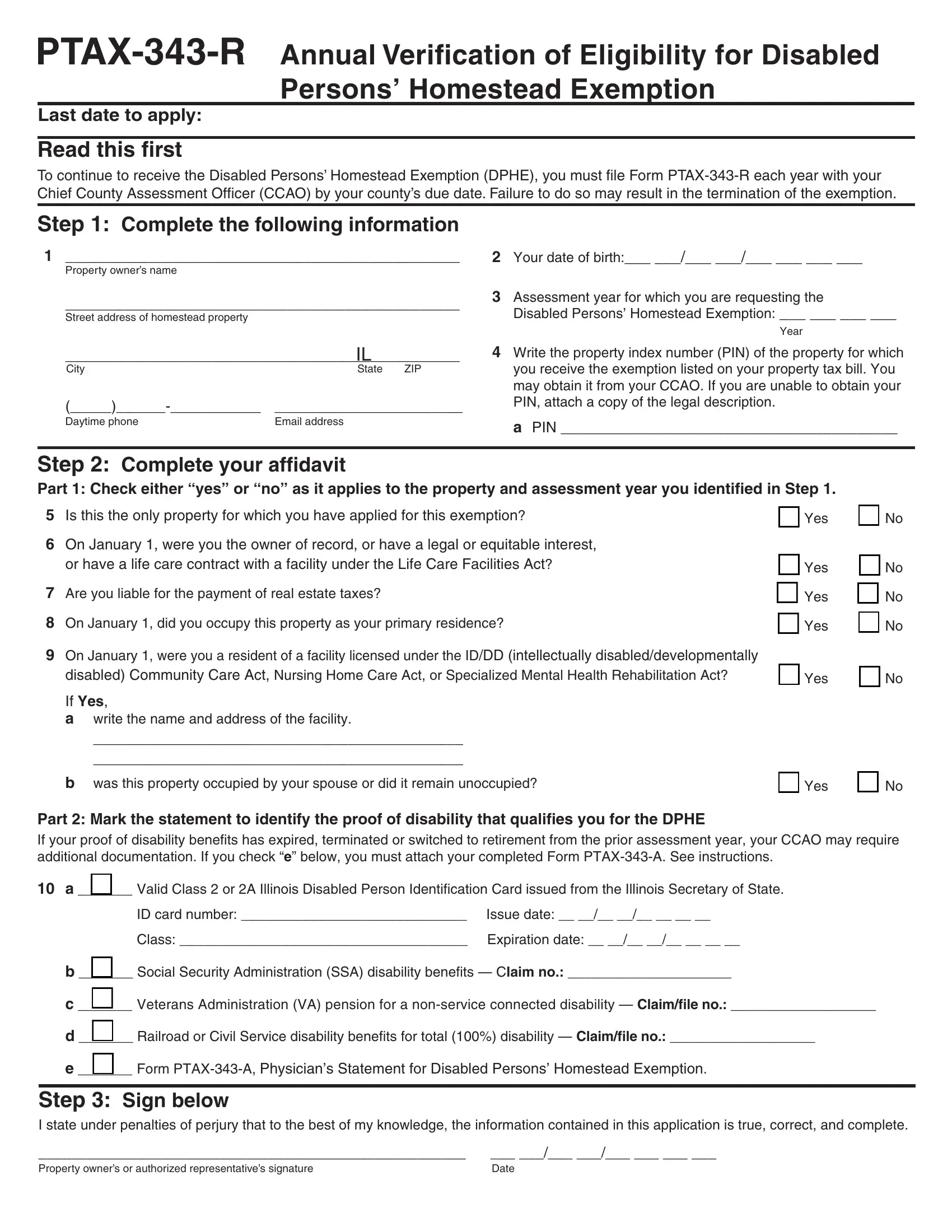
The Form PTAX-343-R, also known as the Annual Verification of Eligibility for Disabled Persons’ Homestead Exemption, serves as a critical piece of documentation for disabled individuals seeking to maintain their homestead exemption benefits annually. To ensure the continued receipt of the Disabled Persons’ Homestead Exemption (DPHE), which offers a $2,000 reduction in the equalized assessed value (EAV) of a property, this form must be duly completed and submitted to the Chief County Assessment Officer (CCAO) by the specified due date of the respective county. The form meticulously gathers essential details such as property owner information, proof of disability, and a declaration of the property's status concerning occupancy and ownership as of January 1 of the assessment year. Additionally, it outlines the requirements for qualifying for the DPHE, inclusive of disability certification, ownership or equitable interest, and liability for property tax payments. Failure to adhere to the annual submission requirement can lead to the forfeiture of the exemption—a scenario that emphasizes the importance of timely and accurate completion of the form. Moreover, it highlights the necessity for applicants to provide up-to-date documentation of their disability, which may involve re-submission of specific forms or obtaining new verification to reflect changes in their condition or disability status from the previous assessment year.
| Question | Answer |
|---|---|
| Form Name | Form Ptax 343 R |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ptax 343 r form, ptax 343 r, 343-A, ptax |

Last date to apply:
Read this first
To continue to receive the Disabled Persons’ Homestead Exemption (DPHE), you must file Form
Step 1: Complete the following information
1________________________________________________
Property owner’s name
________________________________________________
Street address of homestead property
2Your date of birth:___ ___/___ ___/___ ___ ___ ___
3Assessment year for which you are requesting the
Disabled Persons’ Homestead Exemption: ___ ___ ___ ___
Year
|
IL |
City |
State ZIP |
Daytime phone |
Email address |
4Write the property index number (PIN) of the property for which you receive the exemption listed on your property tax bill. You may obtain it from your CCAO. If you are unable to obtain your PIN, attach a copy of the legal description.
a PIN _________________________________________
Step 2: Complete your affidavit
Part 1: Check either “yes” or “no” as it applies to the property and assessment year you identified in Step 1.
5 Is this the only property for which you have applied for this exemption? |
|
Yes |
6On January 1, were you the owner of record, or have a legal or equitable interest,
|
or have a life care contract with a facility under the Life Care Facilities Act? |
|
Yes |
|
7 |
Are you liable for the payment of real estate taxes? |
|
|
Yes |
|
|
|||
8 |
|
|
|
|
On January 1, did you occupy this property as your primary residence? |
|
Yes |
||
9On January 1, were you a resident of a facility licensed under the ID/DD (intellectually disabled/developmentally
disabled) Community Care Act, Nursing Home Care Act, or Specialized Mental Health Rehabilitation Act? |
|
Yes |
If Yes,
awrite the name and address of the facility.
_____________________________________________
_____________________________________________
b was this property occupied by your spouse or did it remain unoccupied? |
|
Yes |
No
No
No
No
No
No
Part 2: Mark the statement to identify the proof of disability that qualifies you for the DPHE
If your proof of disability benefits has expired, terminated or switched to retirement from the prior assessment year, your CCAO may require additional documentation. If you check “e” below, you must attach your completed Form
10a _______ Valid Class 2 or 2A Illinois Disabled Person Identification Card issued from the Illinois Secretary of State.
ID card number: _____________________________ |
Issue date: __ __/__ __/__ __ __ __ |
Class: _____________________________________ |
Expiration date: __ __/__ __/__ __ __ __ |
b _______ Social Security Administration (SSA) disability benefits — Claim no.: _____________________
c _______ Veterans Administration (VA) pension for a
d _______ Railroad or Civil Service disability benefits for total (100%) disability — Claim/file no.: ___________________
e _______ Form
Step 3: Sign below
I state under penalties of perjury that to the best of my knowledge, the information contained in this application is true, correct, and complete.
____________________________________________________ ___ ___/___ ___/___ ___ ___ ___
Property owner’s or authorized representative’s signature |
Date |

Form
What is the Disabled Persons’ Homestead Exemption?
The Disabled Persons’ Homestead Exemption (DPHE) (35 ILCS
Who is eligible?
To qualify for the DPHE you must
•be disabled or have become disabled during the assessment year (i.e., cannot participate in any “substantial gainful activity by reason of a medically determinable physical or mental impairment” which will result in the person’s death or that will last for at least 12 continuous months),
•own or have a legal or equitable interest in the property on which a
•be liable for the payment of the property taxes.
If you previously received the DPHE and now reside in a facility licensed under the ID/DD (intellectually disabled/developmentally disabled) Community Care Act, Nursing Home Care Act, or Spe- cialized Mental Health Rehabilitation Act, you are still eligible to receive the DPHE provided your property
•is occupied by your spouse; or
•remains unoccupied during the assessment year.
If you are a resident of a cooperative apartment building or life care facility as defined under Section 2 of the Life Care Facilities Act (210 ILCS 40/1 et. seq.) you are still eligible to receive the DPHE provided you occupy the property as your primary residence and you are
•liable by contract with the owner(s) of record for the payment of the apportioned property taxes on the property; and
•an owner of record of a legal or equitable interest in the cooperative apartment building. Leasehold interest does not qualify for this exemption.
2Proof of Social Security Administration disability benefits which includes an award letter, verification letter or annual Cost of Living Adjustment (COLA) letter (only COLA Form
Forms
3Proof of Veterans Administration disability benefits which includes an award letter or verification letter indicating you are receiving a pension for a
4Proof of Railroad or Civil Service disability benefits which includes an award letter or verification letter of total (100%) disability.
When will I receive my exemption?
The year you apply (renew) for this exemption is referred to as the assessment year. The County Board of Review while in session for the assessment year has the final authority to grant your exemp- tion. If your exemption is granted, it will be applied to the property tax bill paid the year following the assessment year.
When and where must I file Form
To continue to receive this exemption, you must file
Form
File or mail your completed Form
Madison County, CCAO
157 N Main St Room 229 |
|
|
____________________________________________________ |
||
Mailing address |
|
|
Edwardsville |
IL |
62025 |
City |
|
ZIP |
618 |
692 |
6270 |
If you have any questions, call:
What documentation is required?
Your Chief County Assessment Officer (CCAO) may request you to provide documentation as proof of your disability to continue to qualify for the DPHE. You must provide documentation if your proof of disability has changed or expired from the prior year, including Social Security Administration’s disability benefits that switched over to retirement benefits. The proof of disability must be for the assessment year shown on Line 3 of this application.
If you are unable to provide any of the items listed below as proof of your disability, you must resubmit Form PTAX
1A Class 2 Illinois Disabled Person Identification Card from the Illinois Secretary of State’s Office. Class 2 or Class 2A qualifies for this exemption. Class 1 or 1A does not qualify.
Can I designate another person to receive a property tax delinquency notice for my property?
Yes. Contact your CCAO for information on how to designate an- other person to receive a duplicate of a property tax delinquency notice for your property.
Are there other homestead exemptions available for disabled persons or disabled veterans?
Yes. However, only one of the following disabled homestead exemp- tions may be claimed on your property for a single assessment year
•Disabled Veterans’ Homestead Exemption
•Disabled Persons’ Homestead Exemption
•Disabled Veterans’ Standard Homestead Exemption
|
|
|
|
Official use. Do not write in this space. |
|
||
Date received:___ ___/___ ___/___ ___ ___ ___ |
|
|
Board of review action date: ___ ___/___ ___/___ ___ ___ ___ |
||||
Verify Proof of Disability: |
1 |
2 |
3 |
4 |
Approved |
Denied |
|
Expiration date:___ ___/___ ___/___ ___ ___ ___ |
|
|
Reason for denial ________________________________________ |
||||
Comments:______________________________________________ |
_______________________________________________________ |
||||||
_______________________________________________________ |
_______________________________________________________ |
||||||