
You could complete Form Rad 2944 Lv easily with our PDFinity® editor. We are dedicated to making sure you have the ideal experience with our editor by consistently adding new functions and upgrades. With all of these improvements, working with our tool gets better than ever before! With a few basic steps, you are able to begin your PDF journey:
Step 1: Access the PDF doc in our tool by clicking the "Get Form Button" at the top of this webpage.
Step 2: When you launch the online editor, you will get the document all set to be filled out. Other than filling out various blank fields, you can also perform other actions with the file, specifically writing any words, modifying the initial textual content, inserting illustrations or photos, signing the form, and more.
This PDF form will need you to enter specific details; in order to guarantee correctness, make sure you heed the recommendations further down:
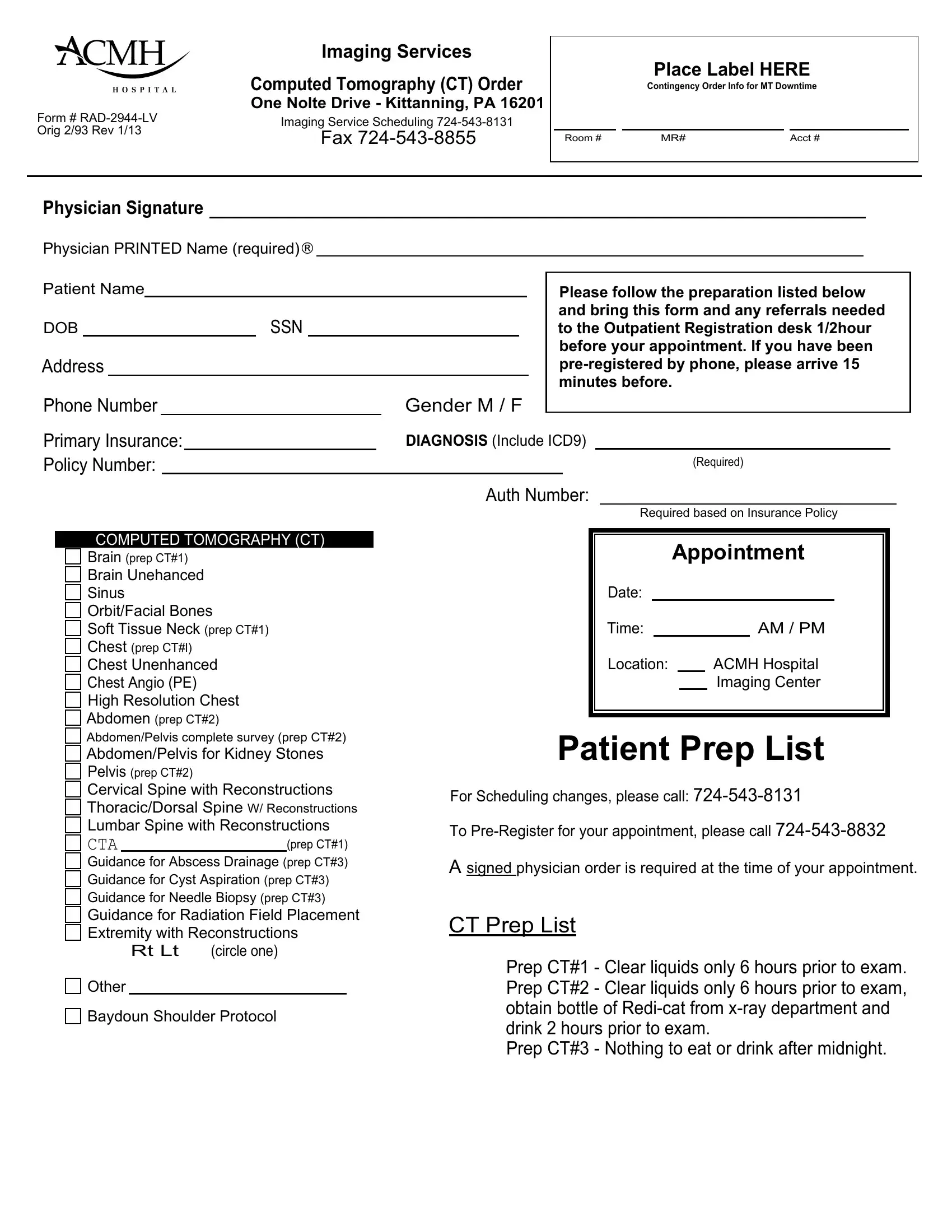
1. The Form Rad 2944 Lv needs certain details to be entered. Be sure that the next fields are complete:
2. After this segment is finished, you should add the required particulars in COMPUTED TOMOGRAPHY CT, Brain prep CT Brain Unehanced, prep CT Guidance for Abscess, Rt Lt, circle one, Other, Appointment, Date, Time, Location, AM PM, ACMH Hospital Imaging Center, Patient Prep List, For Scheduling changes please call, and To PreRegister for your allowing you to go to the 3rd part.
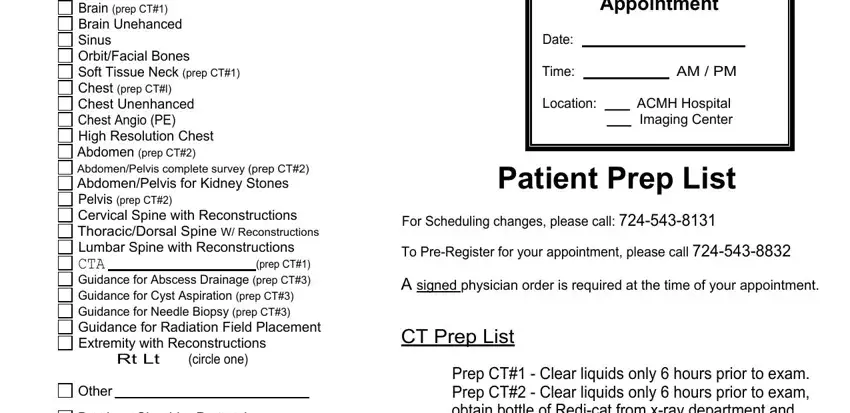
It is possible to make an error when completing the Time, therefore make sure that you reread it prior to when you finalize the form.
Step 3: When you have reread the information entered, press "Done" to finalize your FormsPal process. Make a free trial account with us and obtain instant access to Form Rad 2944 Lv - downloadable, emailable, and editable inside your personal cabinet. We don't share any information that you enter whenever completing forms at our site.