

By using the online PDF editor by FormsPal, you're able to fill in or alter 2817 right here. To make our tool better and easier to utilize, we consistently develop new features, taking into account suggestions coming from our users. Should you be looking to get started, this is what you will need to do:
Step 1: Access the PDF form in our tool by hitting the "Get Form Button" at the top of this webpage.
Step 2: With the help of this advanced PDF editing tool, you may do more than merely fill out blank fields. Express yourself and make your forms seem sublime with customized textual content added in, or fine-tune the file's original input to perfection - all accompanied by an ability to insert your personal pictures and sign the file off.
As for the blank fields of this particular document, here is what you should do:
1. Whenever filling in the 2817, ensure to complete all of the necessary fields in its corresponding section. This will help to speed up the work, allowing for your details to be processed quickly and accurately.
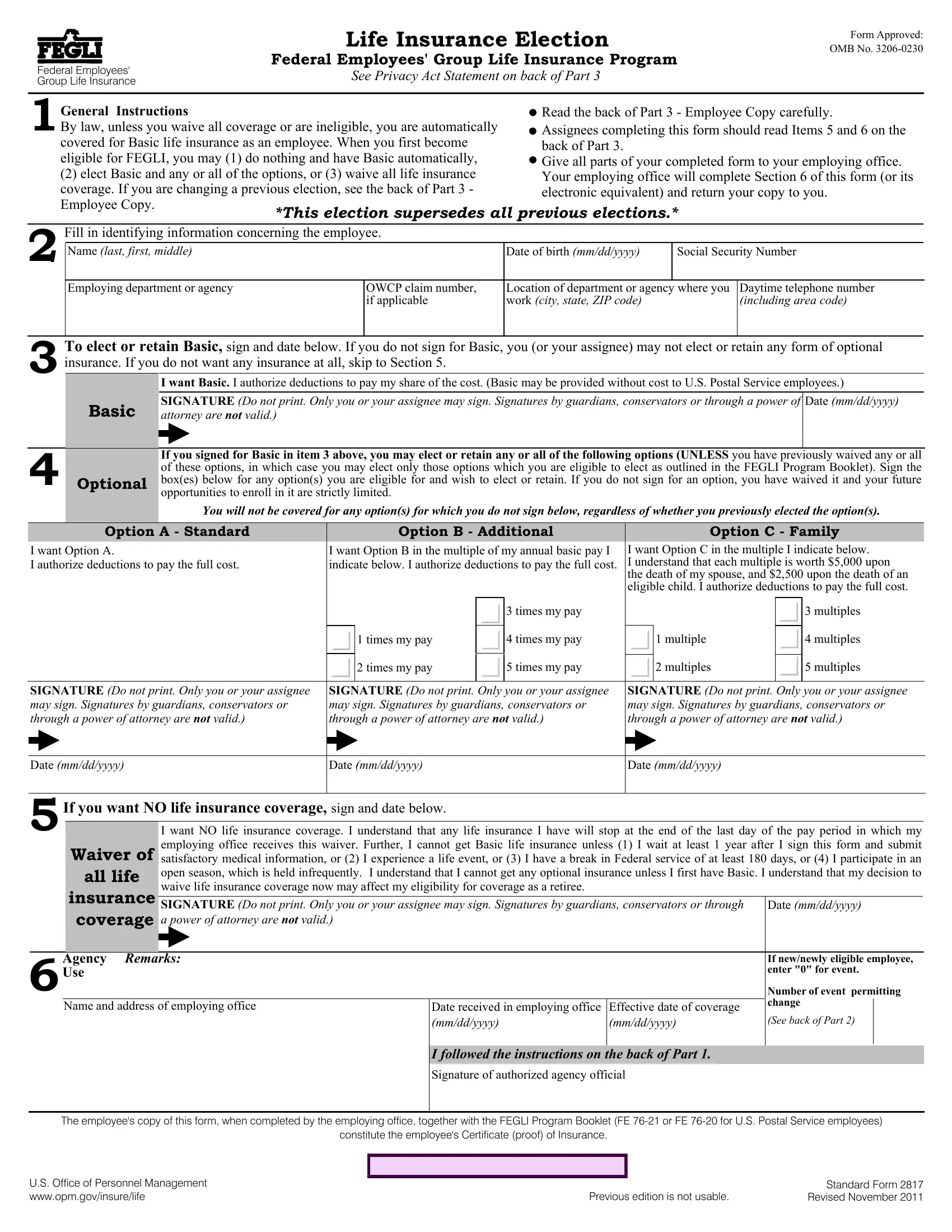
2. Once your current task is complete, take the next step – fill out all of these fields - I want Option C in the multiple I, times my pay, times my pay, times my pay, multiple, times my pay, times my pay, multiples, multiples, multiples, multiples, SIGNATURE Do not print Only you or, SIGNATURE Do not print Only you or, SIGNATURE Do not print Only you or, and Date mmddyyyy with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
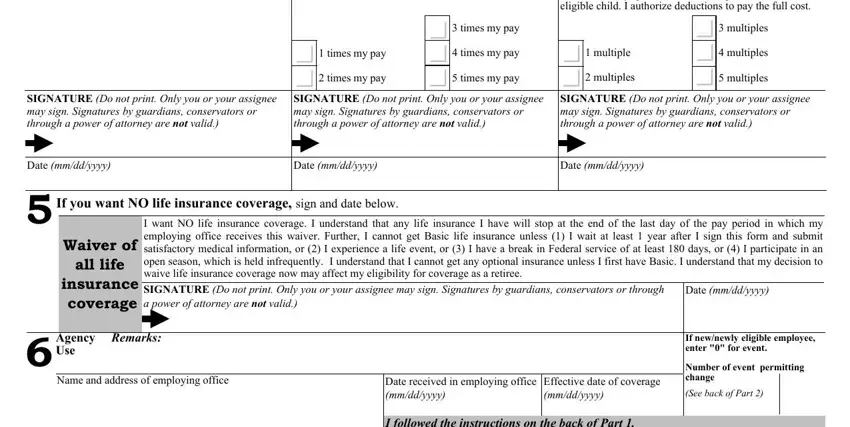
Concerning times my pay and Date mmddyyyy, be certain you get them right in this section. These are definitely the most significant ones in this PDF.
3. This 3rd segment is typically quite easy, Signature of authorized agency, The employees copy of this form, constitute the employees, US Office of Personnel Management, Previous edition is not usable, and Standard Form Revised November - all these fields is required to be completed here.

4. The subsequent part comes next with the following blanks to consider: elect Basic Option A Option B, For Option B and Option C an, Consult the FEGLI Program Booklet, Back of Part, and Standard Form Revised November.
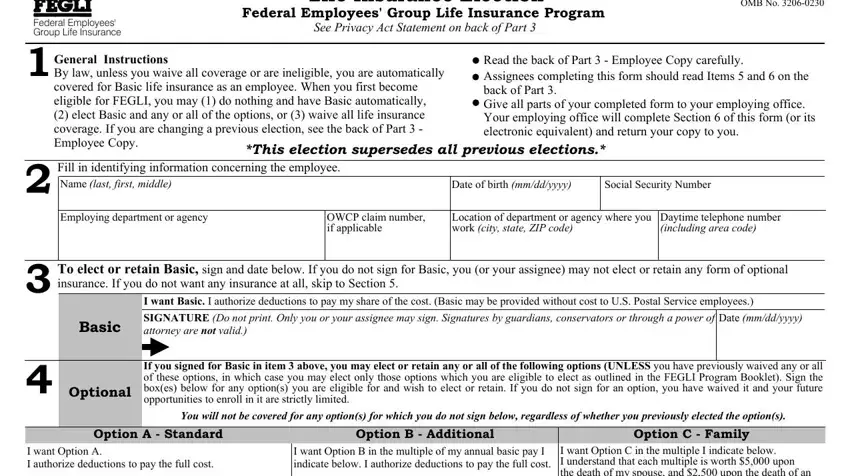
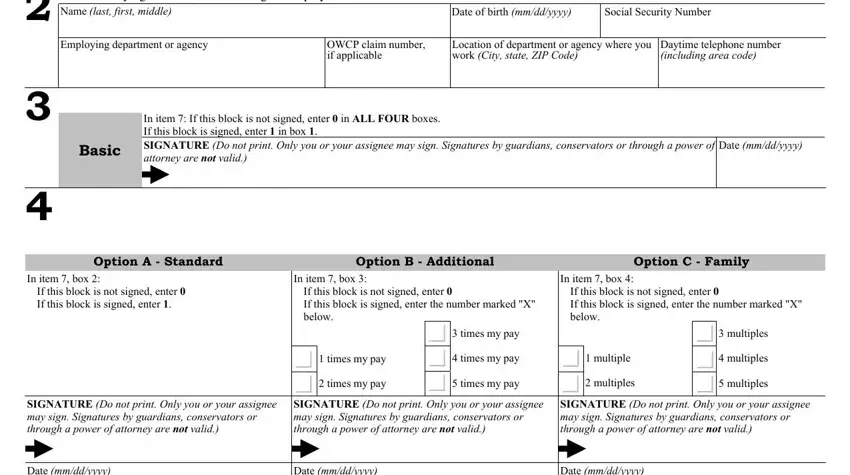
5. To finish your form, this particular part includes several extra blanks. Filling out Fill in identifying information, Name last first middle, Date of birth mmddyyyy, Social Security Number, Employing department or agency, OWCP claim number if applicable, Location of department or agency, Daytime telephone number including, In item If this block is not, Basic, Date mmddyyyy, Option A Standard, Option B Additional, Option C Family, and In item box should wrap up the process and you can be done in a blink!
Step 3: Prior to moving forward, make sure that blank fields were filled out the proper way. When you verify that it's fine, click “Done." Join FormsPal today and instantly access 2817, available for download. Each and every modification made is conveniently preserved , enabling you to change the pdf further when required. Here at FormsPal.com, we strive to make sure that all your details are kept private.