The PDF editor was made with the intention of allowing it to be as effortless and easy-to-use as it can be. The next steps are going to make filling up the Lukes quick and simple.
Step 1: Select the button "Get Form Here" and click it.
Step 2: So, you're on the file editing page. You can add content, edit existing details, highlight specific words or phrases, put crosses or checks, add images, sign the template, erase unneeded fields, etc.
For each area, add the content required by the platform.
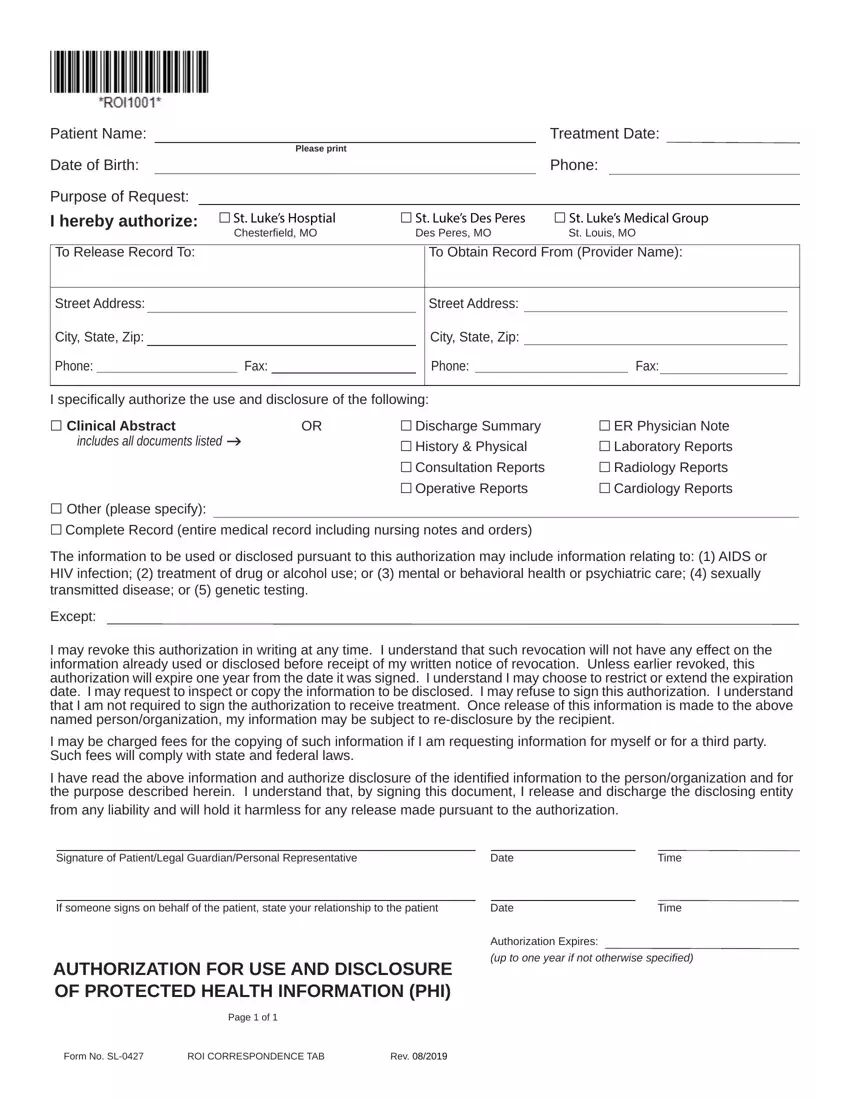
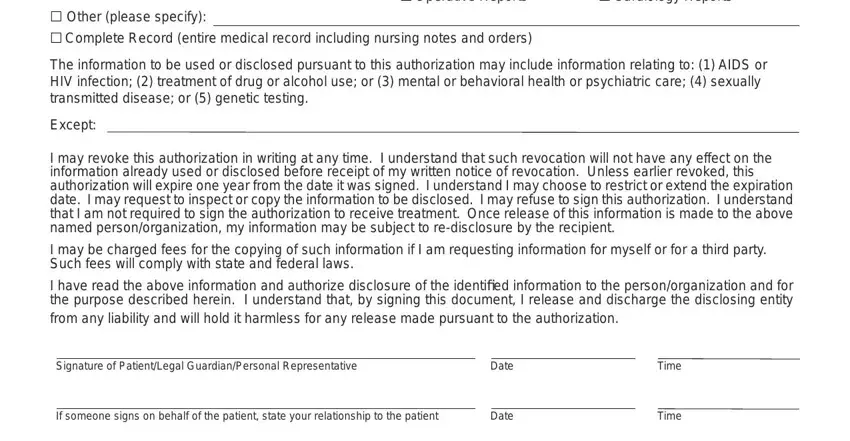
In the part Date, Date, Time, and Time write down the details that the application demands you to do.
Step 3: If you are done, select the "Done" button to export the PDF form.
Step 4: You may create copies of your form toprevent all of the possible future troubles. Don't be concerned, we cannot disclose or check your data.
