
Completing forms with this PDF editor is more straightforward in comparison with anything. To enhance form appointed representative the document, there is nothing you will do - only follow the actions below:
Step 1: Click the button "Get Form Here".
Step 2: The instant you access the form appointed representative editing page, you will see each of the functions it is possible to take regarding your file in the upper menu.
Create the form appointed representative PDF by typing in the content necessary for every single area.
You need to insert the details within the section Additional information regarding, Paperwork Reduction Act Statement, and This information collection meets.
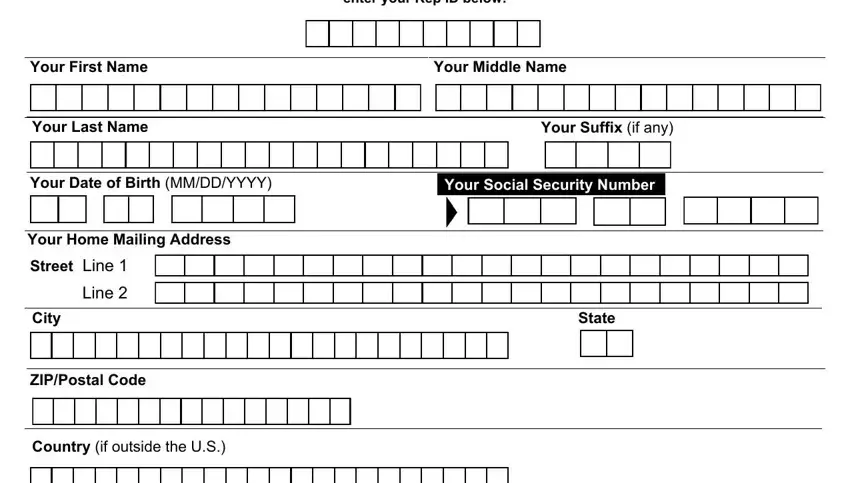
Mention the significant details in If you registered as an Appointed, Your First Name, Your Middle Name, Your Last Name, Your Suffix if any, Your Date of Birth MMDDYYYY, Your Social Security Number, Your Home Mailing Address, Street Line Line, City, ZIPPostal Code, Country if outside the US, and State segment.
Please be sure to include the rights and responsibilities of the sides within the Your Daytime Telephone Number, Your Home Fax Number Optional, CountryArea Code, Phone Number, Extension, CountryArea Code, Fax Number, Your Email Address Optional Used, and Form SSA Destroy Prior Editions box.
Terminate by reading the following areas and preparing them as required: Are you currently in good standing, Yes Go to Section III, No Go to Section IV, NOTE If you are not in the, Section III Your Bar and Court, Provide information for one state, Court or Bar, Year Admitted YYYY, and Court or Bar License Number If one.
Step 3: When you pick the Done button, your finished document is easily transferable to any kind of of your devices. Or, you can deliver it using email.
Step 4: Generate copies of the form - it will help you keep away from future challenges. And don't get worried - we don't distribute or look at your information.
