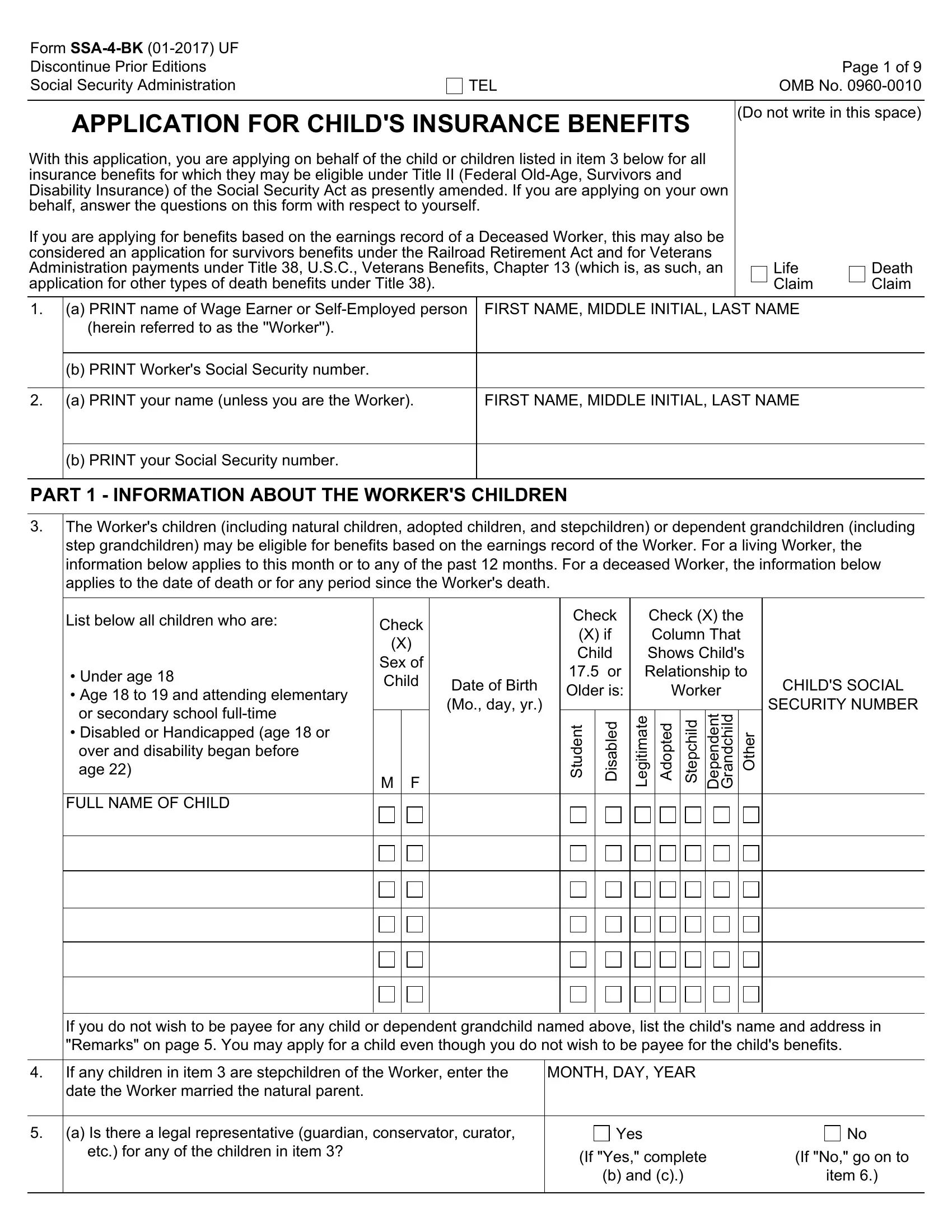
The SSA-4-BK form is a critical document for those seeking to secure Child's Insurance Benefits under Title II of the Social Security Act, which encompasses Federal Old-Age, Survivors, and Disability Insurance. This application facilitates the process for eligible children, including natural, adopted, and stepchildren, as well as dependent grandchildren, to receive benefits based on the earnings record of a living or deceased worker. The form also serves as an application for survivors benefits under the Railroad Retirement Act and for Veterans Administration payments under Veterans Benefits, thus expanding potential assistance beyond social security. Its detailed sections request comprehensive information about the child's relationship to the worker, their residential situation, earning details, and whether previous applications for benefits have been filed. For deceased workers, it gathers essential data regarding the worker's death, military service, and work history, ensuring a thorough evaluation can be completed for entitlement to benefits. Additionally, it addresses the potential need for a legal representative for the child and inquires about any existing conditions that might qualify the child for Supplemental Security Income, underscoring the form’s role in facilitating a broad scope of support for beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 4 Bk |
| Form Length | 9 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 15 sec |
| Other names | social security benefits application form, social security form ssa 4 bk, ssa4 form, social security child insurance |