
 Male
Male
 Female
Female




 -
-
 -
-










 -
-


 -
-




 American Indian or Alaska Native
American Indian or Alaska Native Asian (includes Indian Subcontinent)
Asian (includes Indian Subcontinent) 
 Black or African American
Black or African American
 Hispanic or Latino
Hispanic or Latino
 Native Hawaiian or Other Pacific Islander
Native Hawaiian or Other Pacific Islander
 White
White
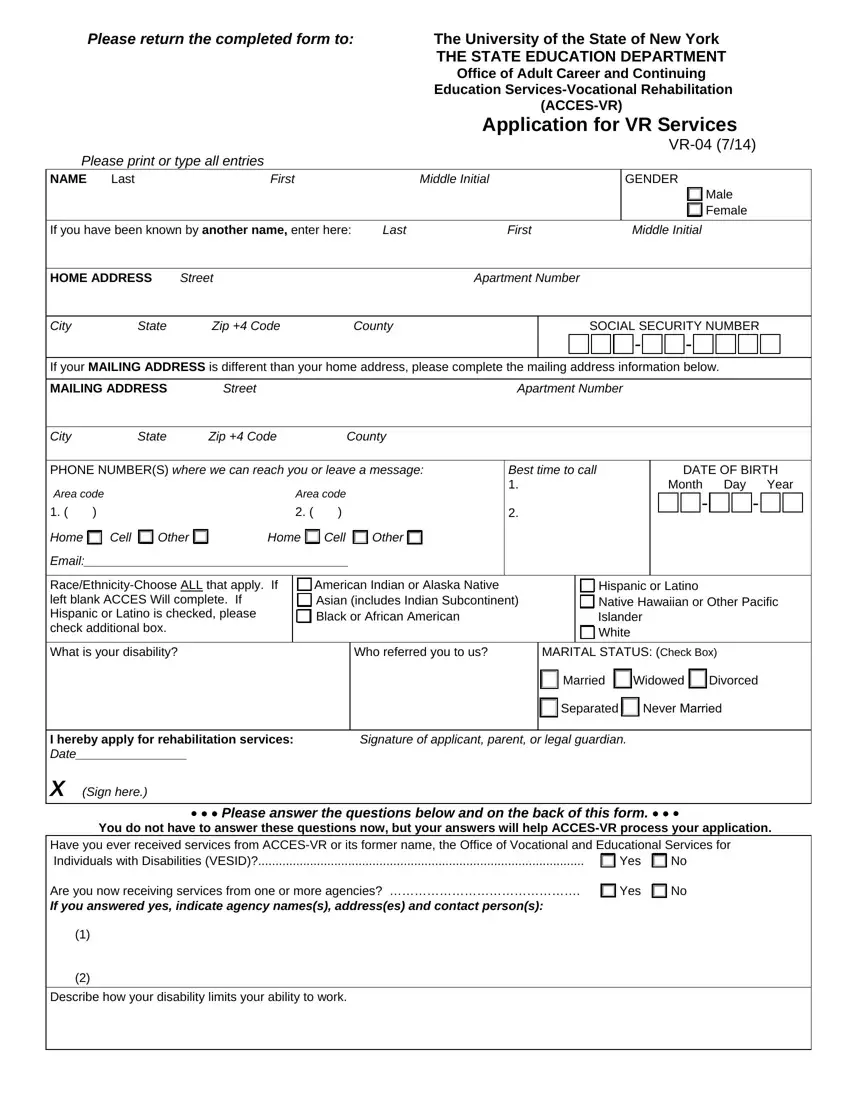
Our finest computer programmers worked hard to set-up the PDF editor we're happy to deliver to you. Our app helps you simply create acces vr application and saves precious time. You only need to comply with this guide.
Step 1: Find the button "Get Form Here" on the following site and press it.
Step 2: Right now, you can start modifying the acces vr application. Our multifunctional toolbar is at your disposal - add, remove, adjust, highlight, and carry out several other commands with the words and phrases in the file.
The next parts are what you are going to fill in to obtain the ready PDF document.
Type in the demanded information in the space Home, Cell, Other, Home, Cell, Other, Email, RaceEthnicityChoose ALL that apply, American Indian or Alaska Native, Hispanic or Latino Native Hawaiian, What is your disability, Who referred you to us, MARITAL STATUS Check Box, Married, and Widowed Divorced.
Identify the valuable information in the Describe how your disability part.

You will have to spell out the rights and responsibilities of both sides in part What services are you seeking from, Are you disabled because of a, Do you use any assistive devices, Do you have a NYS drivers license, Do you have a drivers license from, Do you have Access to a motor, Do you use public transportation, Are you able to leave your home, Yes, Yes, Yes, Yes, Yes, Yes, and Yes.
Finalize by analyzing the next sections and preparing them as needed: List the highest grade you have, GED or High School Equivalency, Yes, College, Graduate School Doctorate, Special Education, Yes, No Do you now attend high school, Yes, Indicate college degrees earned, Name and address of school you, Address, List below other people in your, Full Name, and Age.
Step 3: Hit the "Done" button. At that moment, you may transfer the PDF document - save it to your device or send it through electronic mail.
Step 4: Generate copies of the file - it can help you remain away from possible future problems. And don't worry - we do not publish or view your data.
