Completing inj is easy. Our experts developed our PDF tool to make it simple to use and assist you to prepare any form online. Listed below are steps that you should go through:
Step 1: Choose the "Get Form Here" button.
Step 2: Now, you can start editing your inj. Our multifunctional toolbar is available to you - add, erase, modify, highlight, and carry out similar commands with the text in the file.
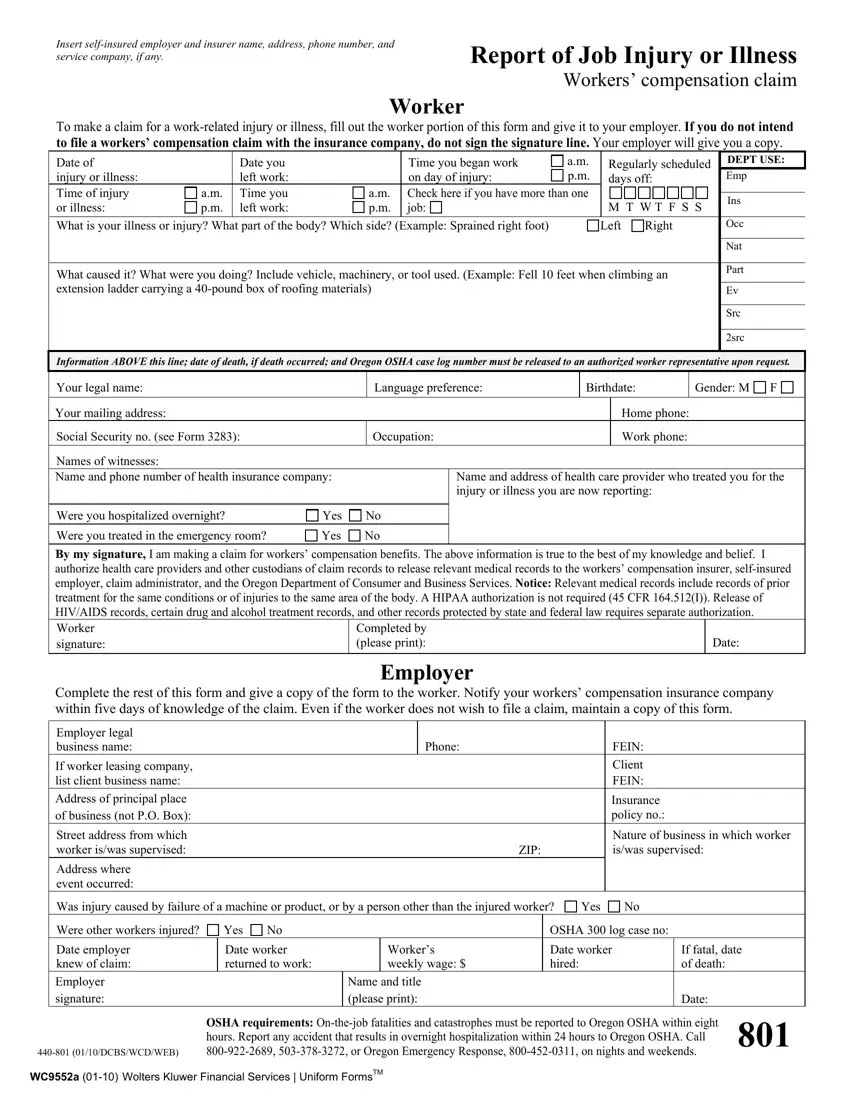
Provide the essential details in each one section to fill out the PDF inj
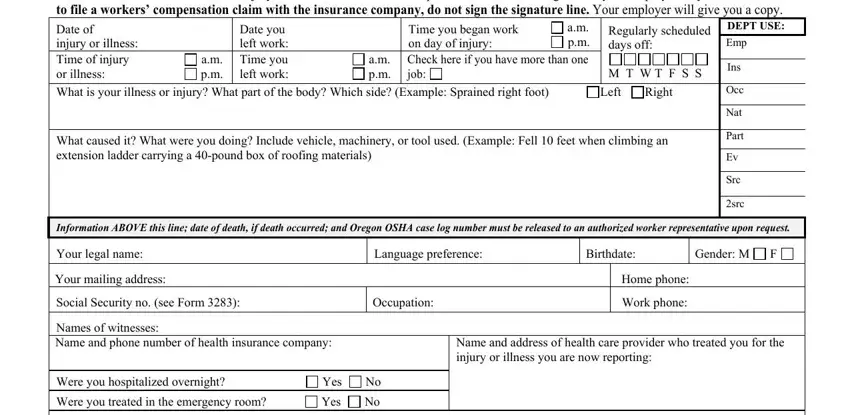
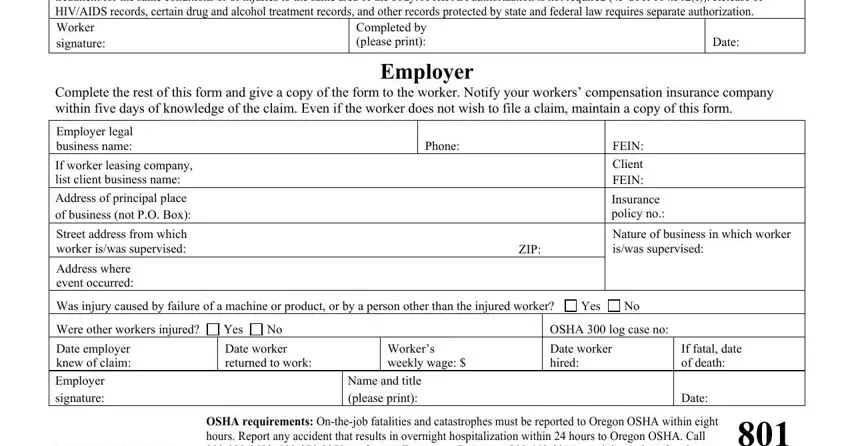
Note the required data in the section Were you treated in the emergency, Completed by please print, Date, Employer, Complete the rest of this form and, Phone, FEIN Client FEIN, Insurance policy no, ZIP, Nature of business in which worker, If worker leasing company list, Street address from which worker, Address where event occurred, Was injury caused by failure of a, and Yes.
Step 3: When you have hit the Done button, your file will be available for export to any electronic device or email you identify.
Step 4: Ensure you keep away from upcoming difficulties by having minimally 2 copies of your form.
