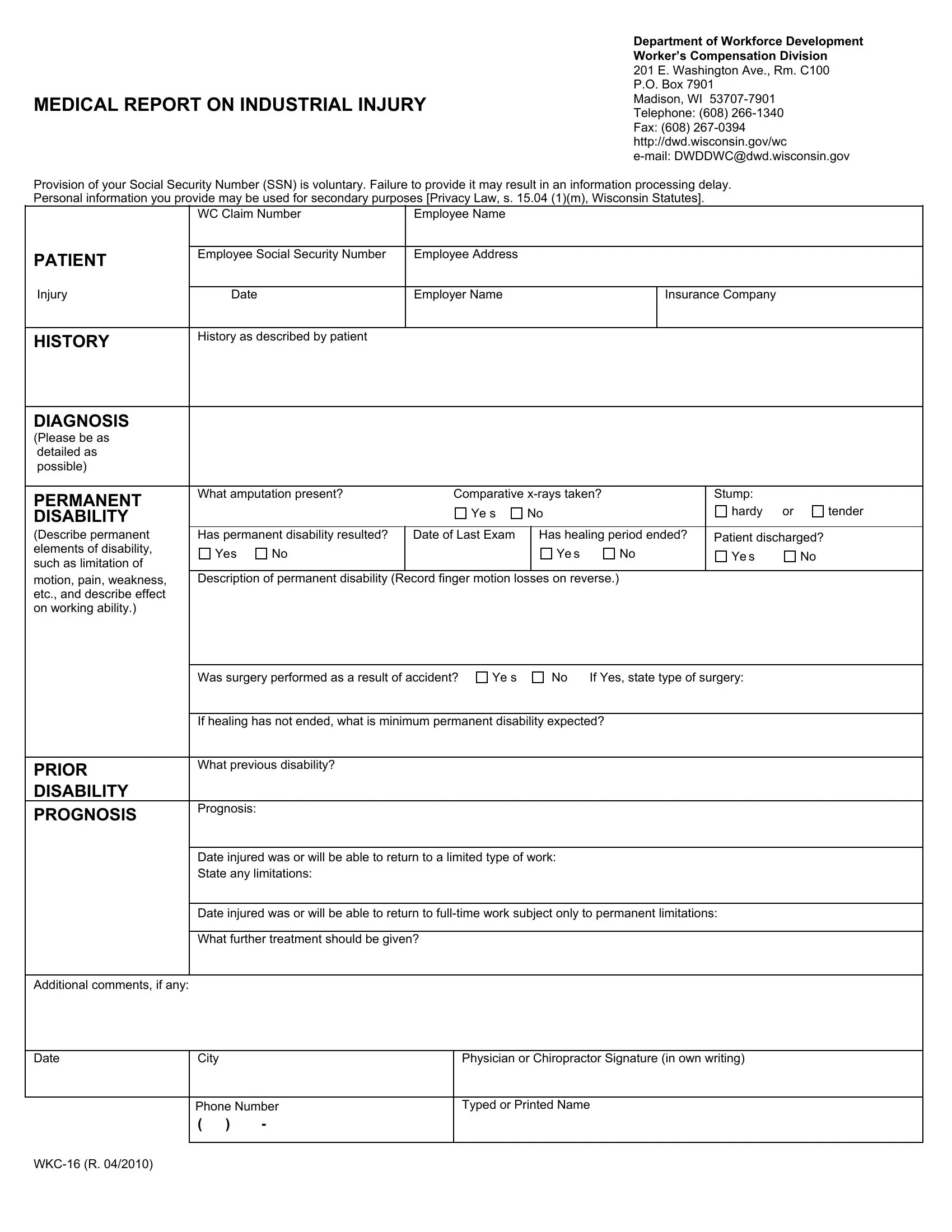
The WKC 16 form, an essential document for the Department of Workforce Development in Wisconsin, plays a pivotal role in the Worker’s Compensation Division process. It is meticulously designed to capture a comprehensive medical report on an industrial injury, ensuring that vital data concerning the worker's condition, the nature of the injury, and the prognosis for recovery are systematically recorded. Situated in Madison, WI, the department handles an array of cases with the primary goal of facilitating the workers' compensation claims efficiently. The form requires detailed information, including personal details of the injured employee, the injury's specifics, diagnosis, and the extent of any permanent disability that may have resulted from the workplace accident. Furthermore, it delves into the history of prior disabilities, if any, and outlines the prognosis for the worker's return to employment, taking into consideration the limitations imposed by the injury. Notably, the form underscores the significance of a thorough evaluation for finger injuries, instructing medical professionals to use statutory terms and precise measurements to assess the loss of use or motion. This meticulous approach to data collection not only aids in the fair assessment of claims but also underscores the department’s commitment to protecting workers’ rights and wellbeing.
| Question | Answer |
|---|---|
| Form Name | Form Wkc 16 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form wkc 16, wkc 16 wisconsin, wkc 16, wkc 16 blank form |