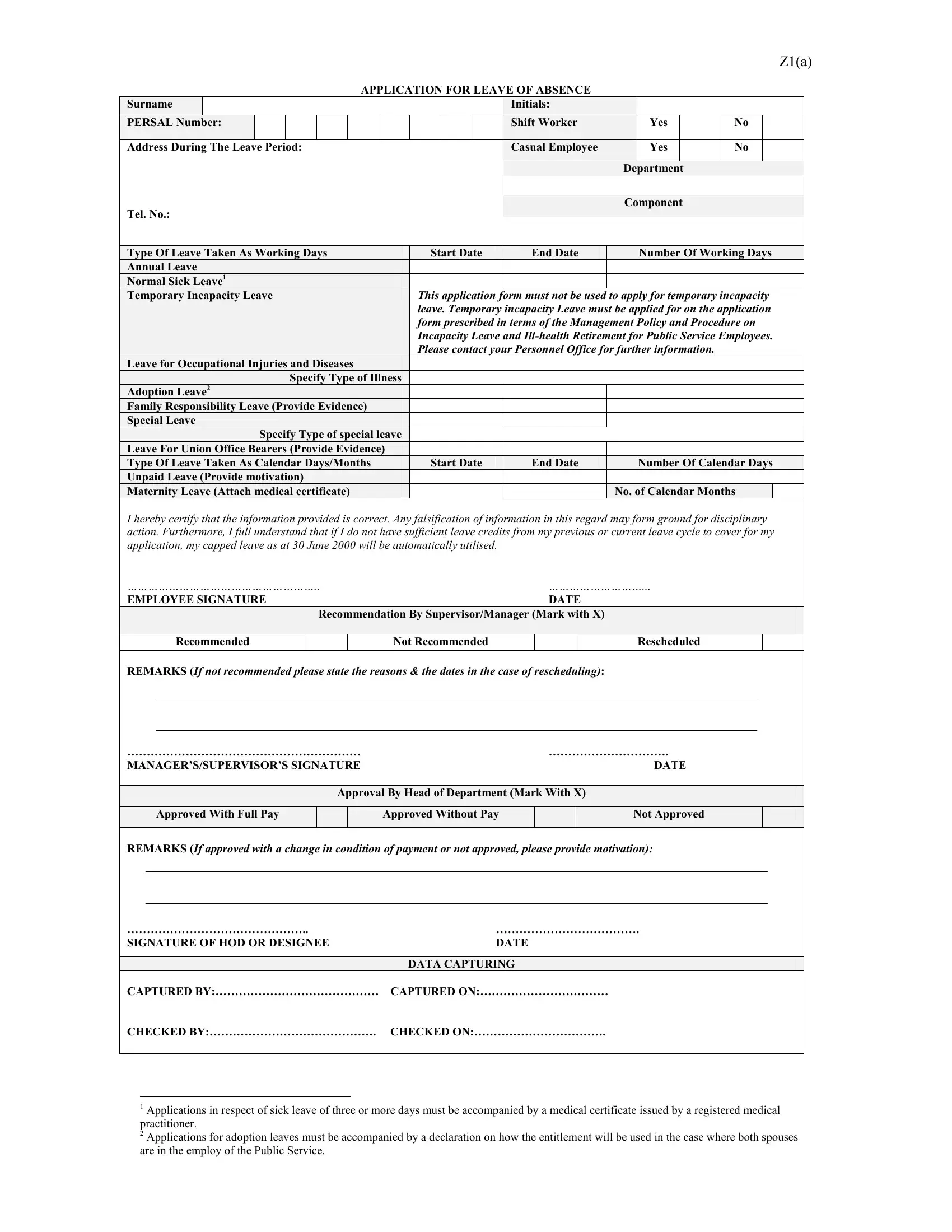
The Z1(a) Application for Leave of Absence is an essential form for employees seeking to take time off from work. This form covers a wide range of leave types including annual leave, normal sick leave, and various specialized leaves such as leave for occupational injuries and diseases, adoption leave, family responsibility leave, special leave, and leave for union office bearers. It is crucial to note that this application must not be used for temporary incapacity leave, for which a different process is prescribed. Employees must provide detailed information such as their surname, initials, PERSAL number, and contact information during the leave period. Furthermore, the form requires specification of the leave type, whether it's being taken as working days or calendar days/months, along with the start and end dates. Applicants must also certify the correctness of the information provided, acknowledging that any falsification may lead to disciplinary action. Additionally, the application includes sections for the recommendation by a supervisor or manager, approval by the head of department with details on the condition of payment, and finally, notes on data capturing. It’s designed to ensure that all applications are thoroughly reviewed and processed in accordance with the Management Policy and Procedure on Incapacity Leave and Ill-health Retirement for Public Service Employees. The Z1(a) form is a critical tool for managing leave, ensuring both employee and employer needs are met with transparency and accountability.
| Question | Answer |
|---|---|
| Form Name | Form Z1 A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | z1 leave form 2021, dpsa leave form, leave form dpsa, dpsa leave form 2021 |
Z1(a)
APPLICATION FOR LEAVE OF ABSENCE
|
Surname |
|
|
|
|
|
|
|
|
|
Initials: |
|
|
|
|
|
|
|
PERSAL Number: |
|
|
|
|
|
|
|
|
Shift Worker |
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address During The Leave Period: |
|
|
|
Casual Employee |
|
Yes |
|
No |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Department |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Component |
|
|
|
||
|
Tel. No.: |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|||||||||||
|
Type Of Leave Taken As Working Days |
Start Date |
End Date |
|
Number Of Working Days |
||||||||||||
|
Annual Leave |
|
|
|
|
|
|
|
|
|
|
||||||
|
Normal Sick Leave1 |
|
|
|
|
|
|
|
|
|
|
||||||
|
Temporary Incapacity Leave |
This application form must not be used to apply for temporary incapacity |
|||||||||||||||
|
|
|
|
|
|
|
|
leave. Temporary incapacity Leave must be applied for on the application |
|||||||||
|
|
|
|
|
|
|
|
form prescribed in terms of the Management Policy and Procedure on |
|||||||||
|
|
|
|
|
|
|
|
Incapacity Leave and |
|||||||||
|
|
|
|
|
|
|
|
Please contact your Personnel Office for further information. |
|
|
|
||||||
|
Leave for Occupational Injuries and Diseases |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
Specify Type of Illness |
|
|
|
|
|
|
|
|
|
|
|||
|
Adoption Leave2 |
|
|
|
|
|
|
|
|
|
|
||||||
|
Family Responsibility Leave (Provide Evidence) |
|
|
|
|
|
|
|
|
|
|
||||||
|
Special Leave |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
Specify Type of special leave |
|
|
|
|
|
|
|
|
|
|
||||
|
Leave For Union Office Bearers (Provide Evidence) |
|
|
|
|
|
|
|
|
|
|
||||||
|
Type Of Leave Taken As Calendar Days/Months |
Start Date |
End Date |
|
Number Of Calendar Days |
||||||||||||
|
Unpaid Leave (Provide motivation) |
|
|
|
|
|
|
|
|
|
|
||||||
|
Maternity Leave (Attach medical certificate) |
|
|
|
|
No. of Calendar Months |
|
||||||||||
I hereby certify that the information provided is correct. Any falsification of information in this regard may form ground for disciplinary action. Furthermore, I full understand that if I do not have sufficient leave credits from my previous or current leave cycle to cover for my application, my capped leave as at 30 June 2000 will be automatically utilised.
……………………………………………….. |
|
………………………... |
||||||||||
EMPLOYEE SIGNATURE |
|
DATE |
|
|
|
|
||||||
|
|
|
|
Recommendation By Supervisor/Manager (Mark with X) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recommended |
|
|
|
Not Recommended |
|
|
Rescheduled |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REMARKS (If not recommended please state the reasons & the dates in the case of rescheduling): |
|
|
|
|
||||||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
…………………………………………………… |
|
…………………………. |
||||||||||
MANAGER’S/SUPERVISOR’S SIGNATURE |
|
|
|
DATE |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Approval By Head of Department (Mark With X) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Approved With Full Pay |
|
|
|
Approved Without Pay |
|
|
Not Approved |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REMARKS (If approved with a change in condition of payment or not approved, please provide motivation): |
||||||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
……………………………………….. |
………………………………. |
|||||||||||
SIGNATURE OF HOD OR DESIGNEE |
DATE |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
DATA CAPTURING |
|
|
|
|
||
CAPTURED BY:…………………………………… |
CAPTURED ON:…………………………… |
|
|
|
|
|||||||
CHECKED BY:……………………………………. |
CHECKED ON:……………………………. |
|
|
|
|
|||||||
1Applications in respect of sick leave of three or more days must be accompanied by a medical certificate issued by a registered medical
practitioner.
2 Applications for adoption leaves must be accompanied by a declaration on how the entitlement will be used in the case where both spouses are in the employ of the Public Service.