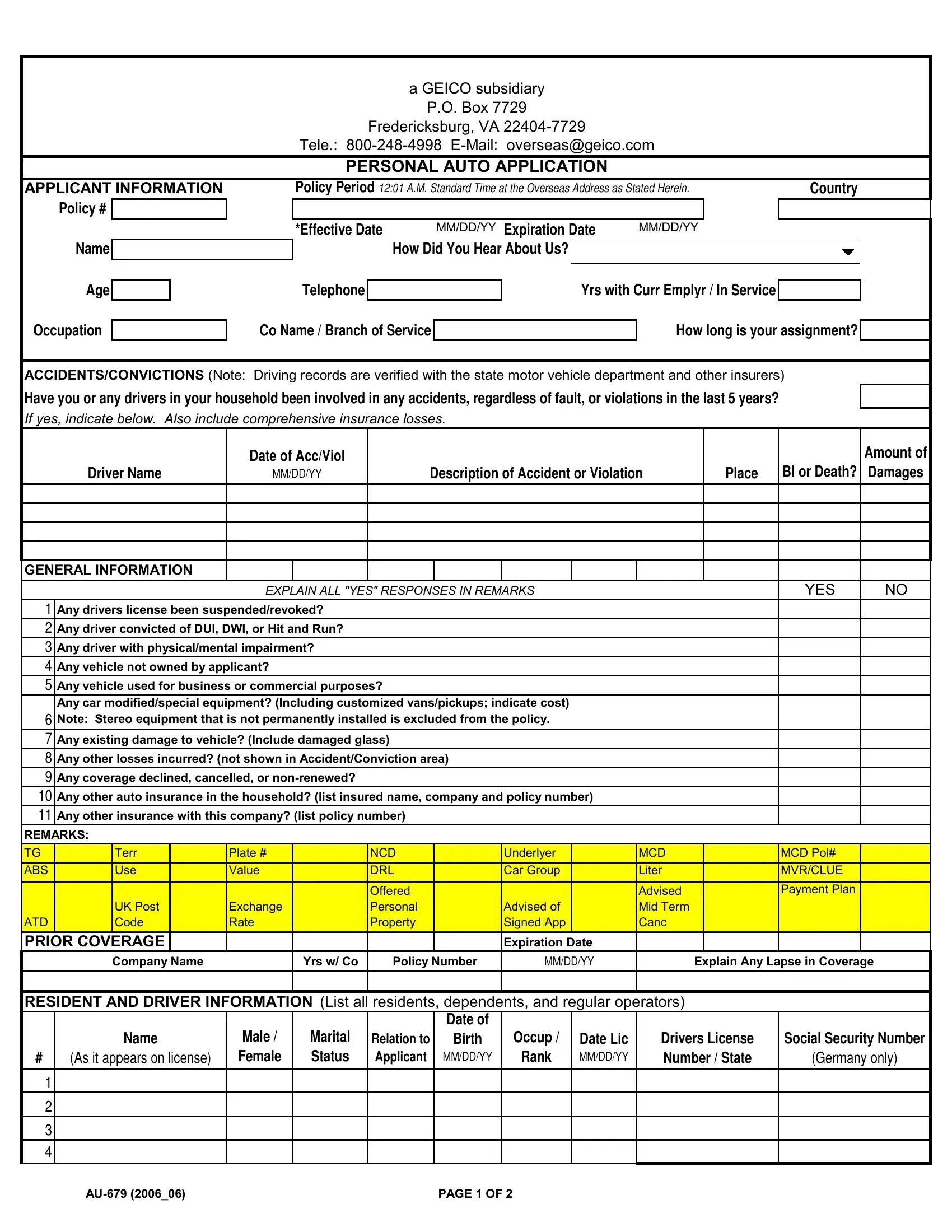
In the realm of auto insurance, the Geico AU 679 form represents a crucial document for those seeking personal auto coverage through a Geico subsidiary. Originating from Fredericksburg, VA, this form serves as a personal auto application and encapsulates a variety of information crucial for the insurance underwriting process. Applicants are required to provide comprehensive details about themselves, including personal information, vehicle data, and driving history, encompassing accidents and convictions within the past five years, to ensure accurate assessment by Geico. Key sections of the form delve into driver's license status, DUI or DWI convictions, physical or mental impairments affecting driving abilities, and the use of vehicles for business purposes. It also probes into any modifications to vehicles, existing damages, loss history, and previous insurance coverages, which collectively inform Geico’s decision-making process. The form underscores the importance of honesty in disclosures, with a clear indication that inaccuracies can lead to policy voidance. Furthermore, it outlines coverage options and premiums, stressing the policy's effective dates and the conditions under which policies can be cancelled or renewed. With spaces for applicant remarks and detailed vehicle and driver information, the AU 679 form is tailored to gather exhaustive data to facilitate a tailored insurance proposal, revealing Geico's methodical approach in offering personal auto insurance.
| Question | Answer |
|---|---|
| Form Name | Geico Form Au 679 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | geico insurance claim, why does geico require paper application, geico claim number, geico insurance claims |