There isn't anything difficult about filling out the generic request form for video once you start using our editor. By taking these easy steps, you'll get the ready PDF file in the least time period you can.
Step 1: Look for the button "Get Form Here" and press it.
Step 2: Now you are going to be on your form edit page. You can include, update, highlight, check, cross, include or erase fields or words.
You will have to type in the next data if you need to complete the file:
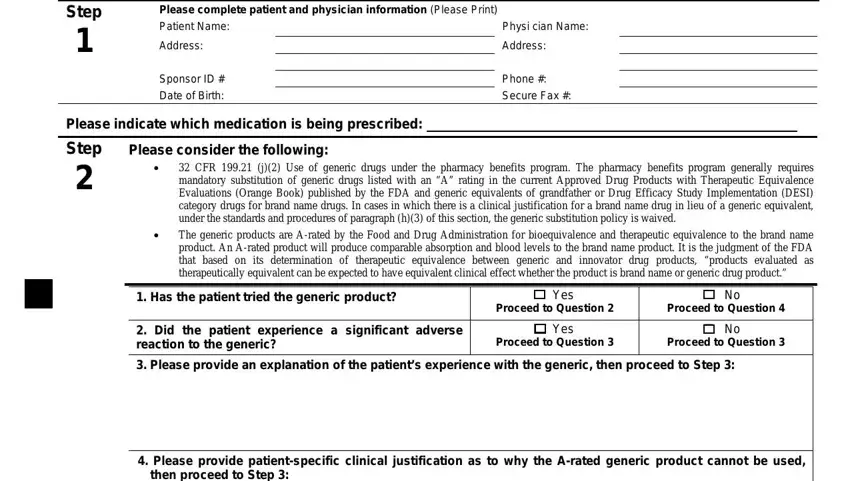
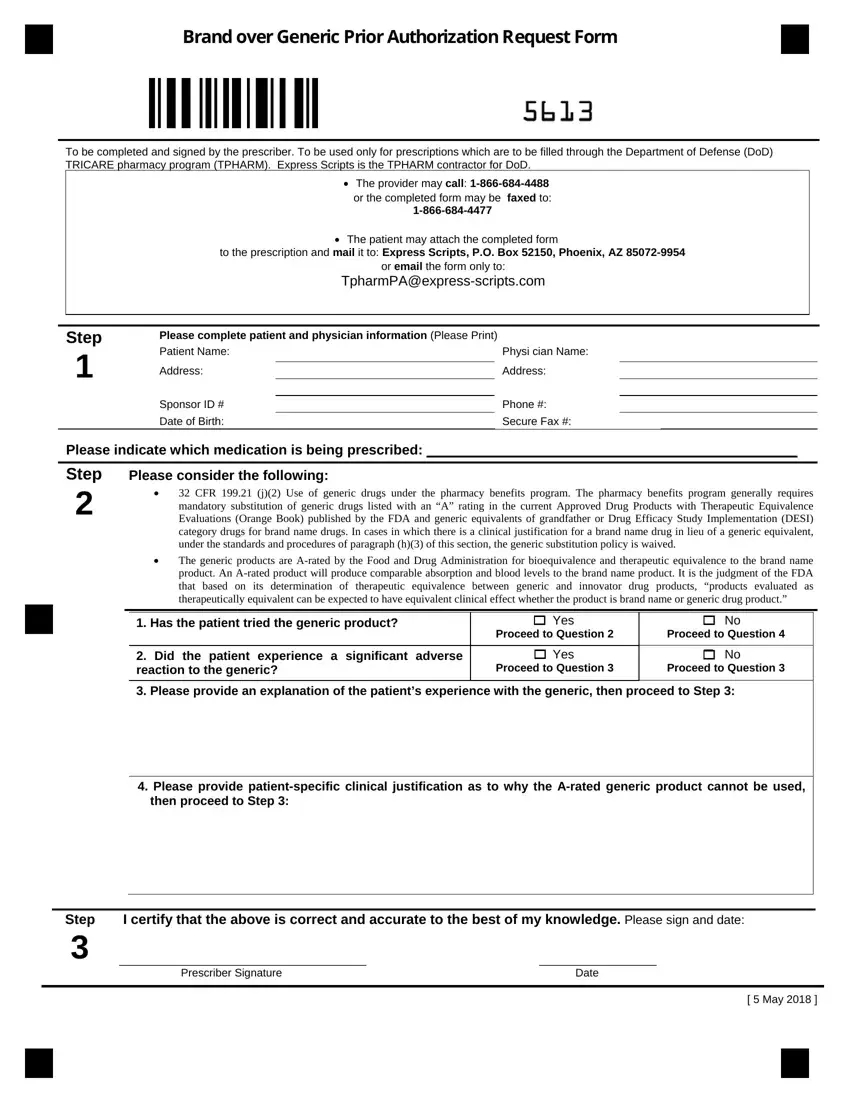
Within the segment Step, Prescriber Signature Date, and May enter the data that the system asks you to do.
Step 3: Press the Done button to assure that your finalized form could be transferred to every electronic device you decide on or forwarded to an email you specify.
Step 4: You will need to make as many duplicates of the document as possible to remain away from future issues.
