
Georgia Department Of Labor Form can be completed easily. Simply open FormsPal PDF editing tool to finish the job without delay. Our expert team is relentlessly endeavoring to develop the editor and help it become even easier for users with its extensive functions. Discover an constantly progressive experience now - take a look at and uncover new opportunities as you go! All it requires is a couple of basic steps:
Step 1: Just press the "Get Form Button" in the top section of this webpage to start up our form editor. There you'll find everything that is needed to fill out your file.
Step 2: The tool enables you to work with your PDF in many different ways. Transform it by including your own text, correct existing content, and include a signature - all at your disposal!
This PDF doc will involve some specific information; in order to guarantee correctness, please make sure to take heed of the next tips:
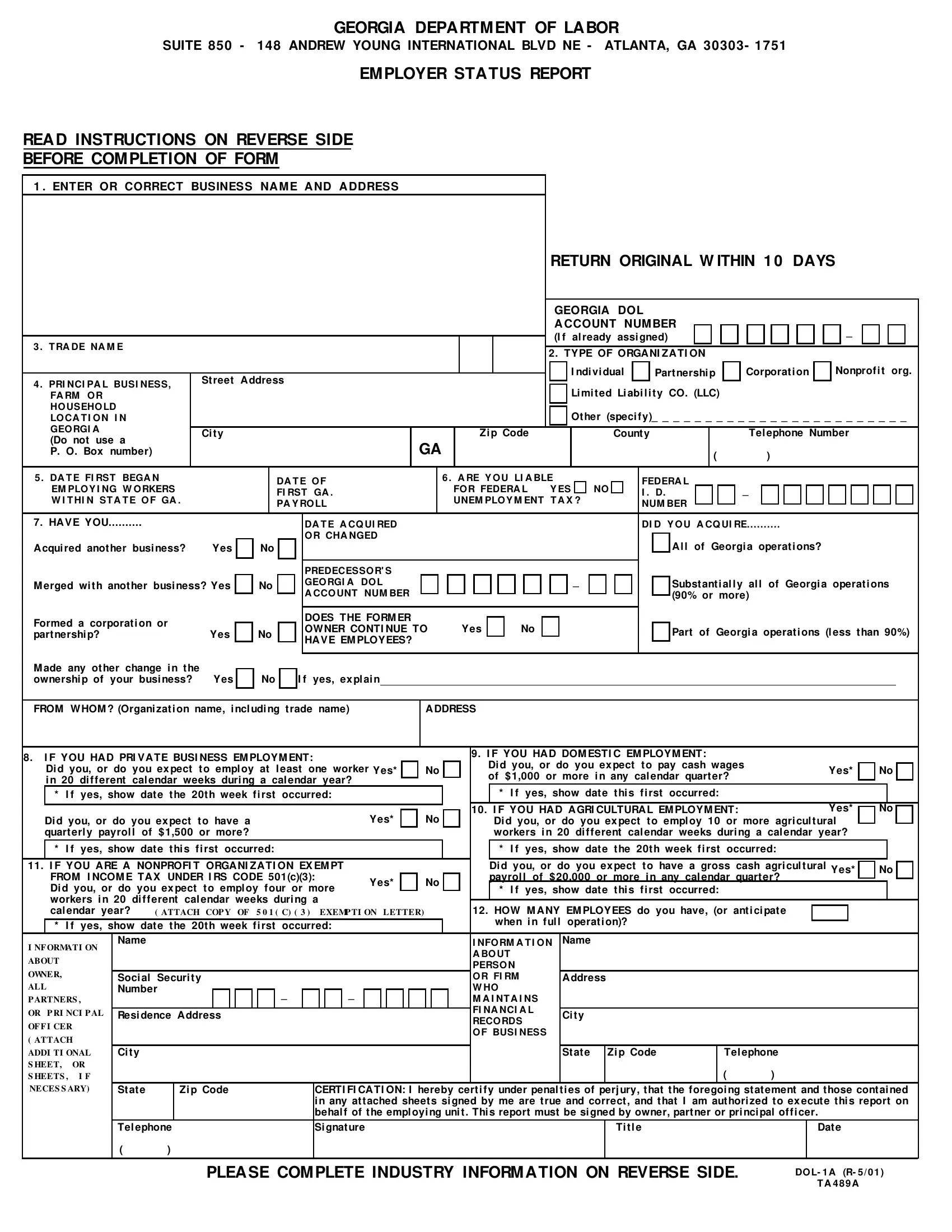
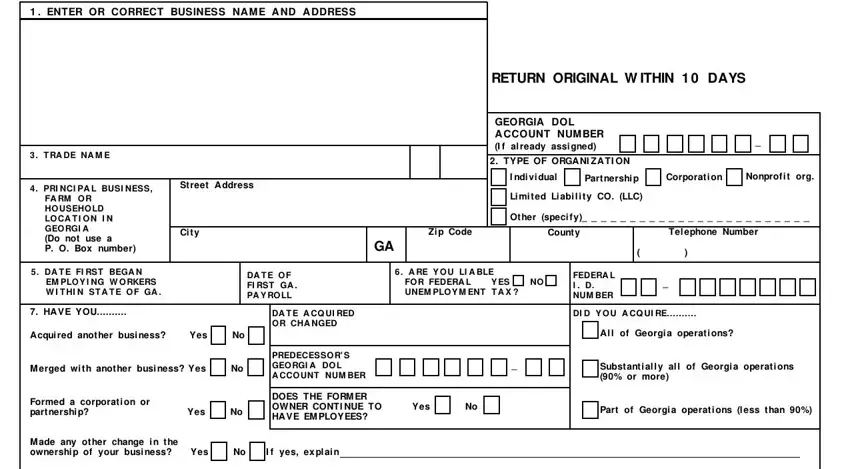
1. To begin with, while filling out the Georgia Department Of Labor Form, start out with the form section that features the next blank fields:
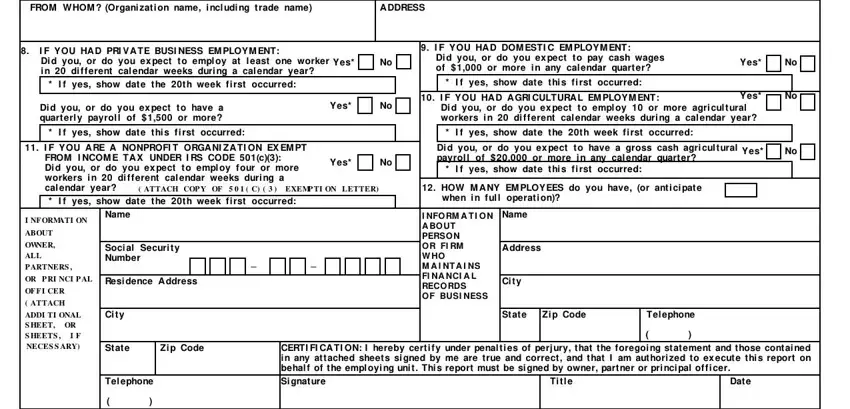
2. Just after finishing this section, head on to the subsequent part and fill out the essential particulars in these blanks - FROM WHOM Organi zati on name i, A DDRESS, I F YOU HA D PRI VA TE BUSI NESS, I f yes show date the th week fi, I F YOU HA D DOM ESTI C EM PLOYM, I f yes show date thi s fi rst, Yes, Di d you or do you ex pect to have, I f yes show date thi s fi rst, I F YOU A RE A NONPROFI T ORGA NI, I f yes show date the th week fi, ATTACH COP Y OF C EXEMP TI, Yes, I F YOU HA D A GRI CULTURA L EM, and Yes.
3. This third step is generally easy - fill out every one of the fields in NATURE OF BUSINESS Inf ormation is, A How many Georgia locations do, Provide the f ollow ing inf, B Check the box that best, business activities, Agriculture Forestry Fishing, Manuf acturing Transportation, C Enter in order of importance and, approximate of total annual, Principal Products Mf g Grow n Sold, this report, I f Transportati on Trucki ng i, If perf orm services f or other, includes establishments, and the company to complete this segment.
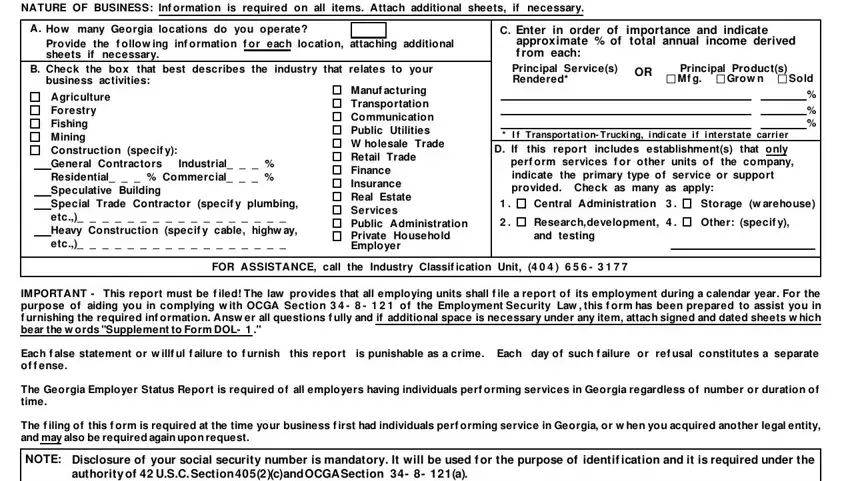
Always be extremely attentive when completing If perf orm services f or other and Provide the f ollow ing inf, as this is where a lot of people make errors.
Step 3: Before obtaining the next step, it's a good idea to ensure that all form fields were filled in right. When you think it is all good, click “Done." Join FormsPal right now and immediately use Georgia Department Of Labor Form, set for download. All adjustments you make are preserved , making it possible to edit the form at a later point if necessary. FormsPal provides safe form editor devoid of personal data recording or distributing. Be assured that your details are safe with us!