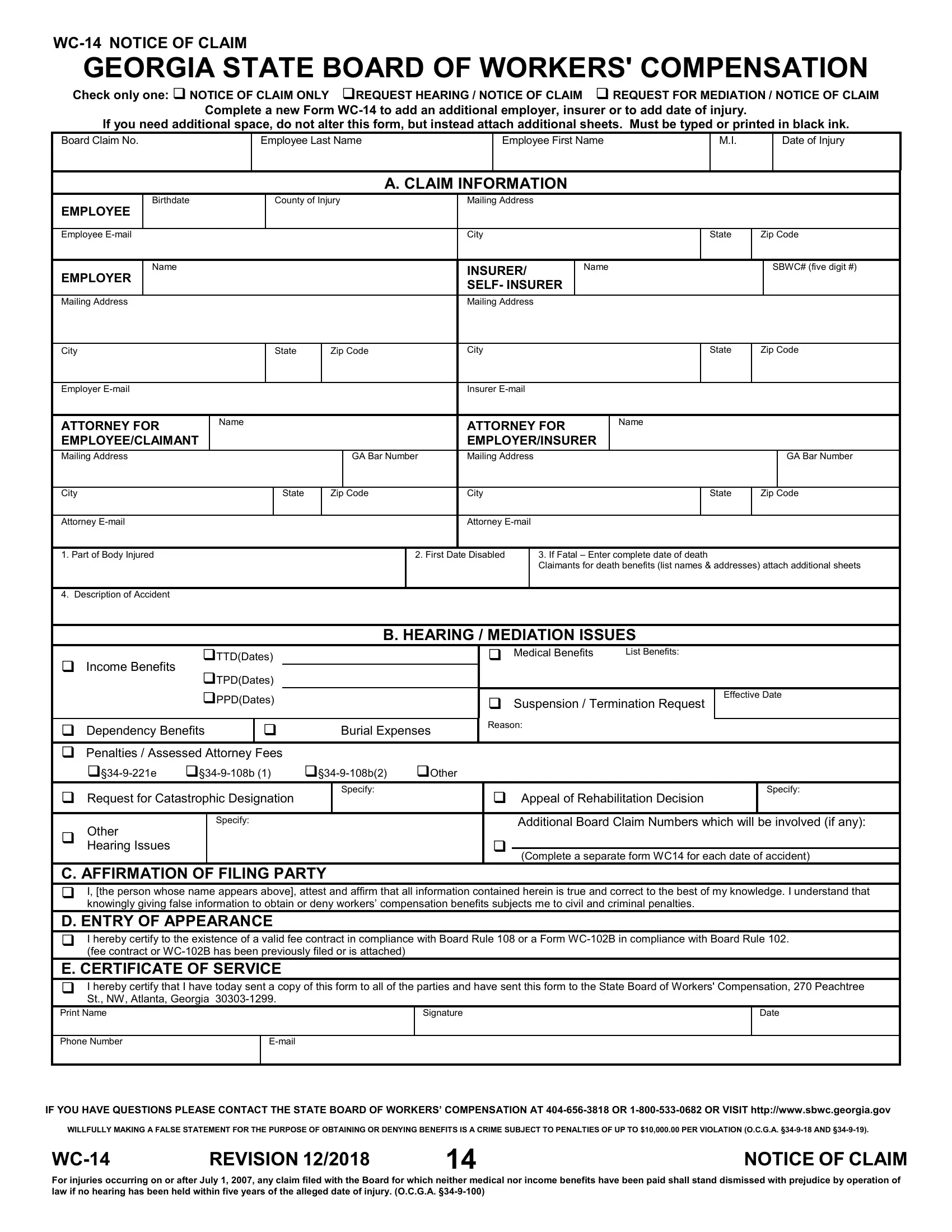
Understanding the intricacies of workers' compensation in Georgia is crucial for employees who find themselves injured on the job. Central to this process is the Form WC-14, also known as the "Notice of Claim." This form serves multiple purposes; it's used not only to notify the Georgia State Board of Workers' Compensation about an injury but also to request a hearing or mediation if necessary. It's a vital step in the claims process, ensuring the injured party's details, including name, date of injury, and a description of the accident, are formally documented. Moreover, it distinguishes between simply notifying about a claim and actively seeking a hearing or mediation, providing spaces to detail the nature of the injury, any dependents for death benefits, and issues for consideration like medical benefits and income benefits. Completeness and accuracy are paramount, as additional sheets can be attached if more space is needed without altering the form itself. The form emphasizes the legal responsibilities of the filing party, including the affirmation of truthfulness under penalty of civil and criminal consequences for falsehoods and the necessity of a certificate of service, confirming the form has been distributed to relevant parties. This article introduces readers to the foundational aspects of the WC-14 form, exploring its purpose, requirements, and significance in the broader workers' compensation claim process in Georgia.
| Question | Answer |
|---|---|
| Form Name | Georgia Wc 14 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wc 14 form, georgia form sbwc, wc 4 georgia, wc 14 |