Completing documents with our PDF editor is simpler in comparison with most things. To modify ARIZONA the file, there is little you need to do - simply adhere to the steps listed below:
Step 1: Hit the button "Get form here" to access it.
Step 2: When you enter our ARIZONA editing page, you will see each of the options you may undertake with regards to your document in the top menu.
Fill in the next parts to create the template:
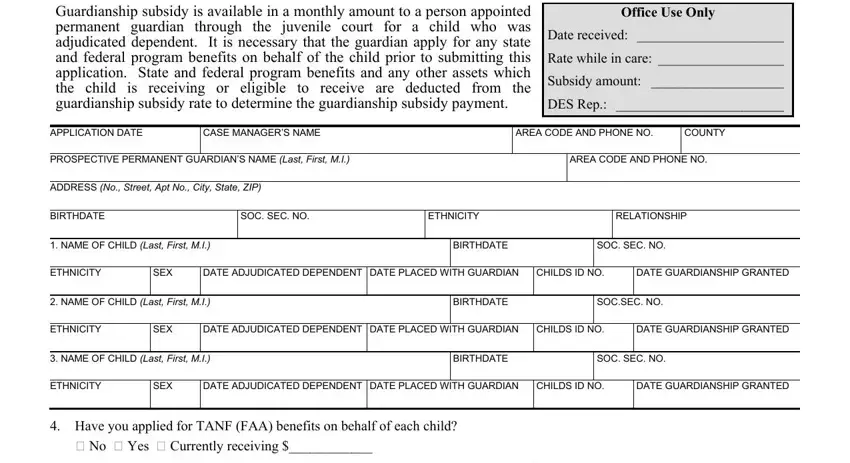
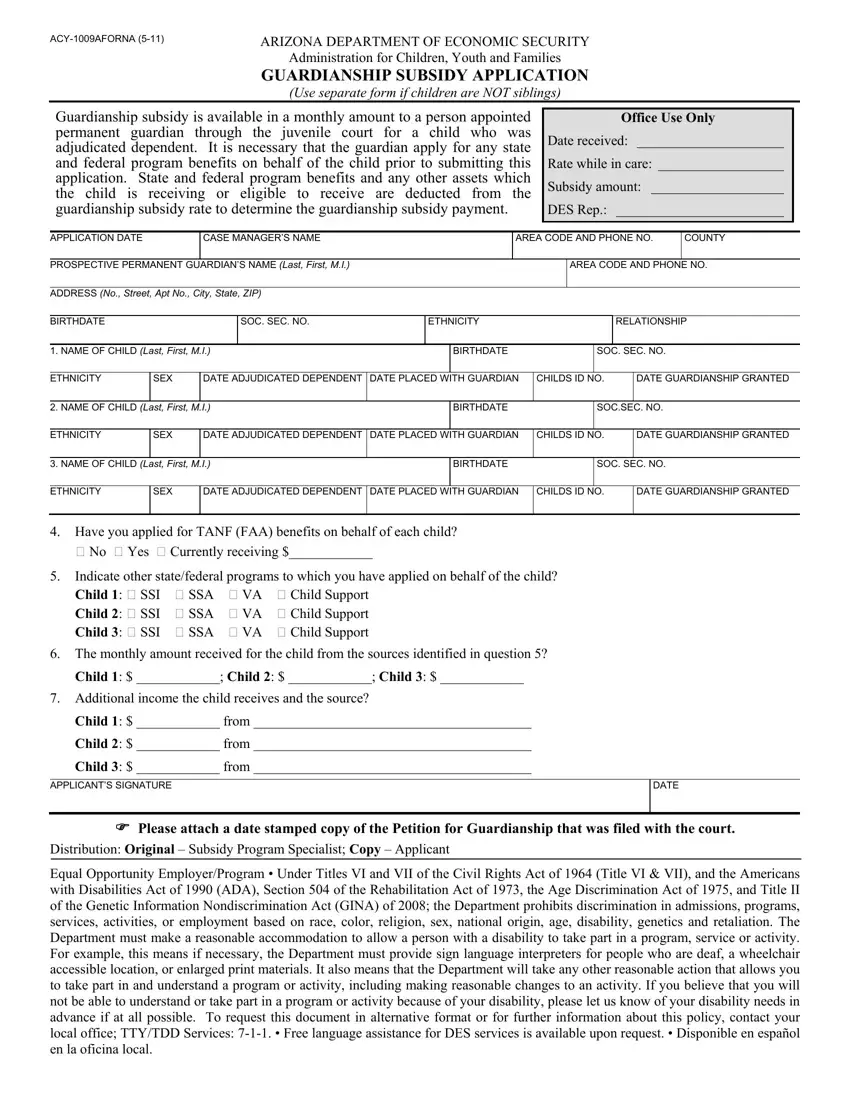
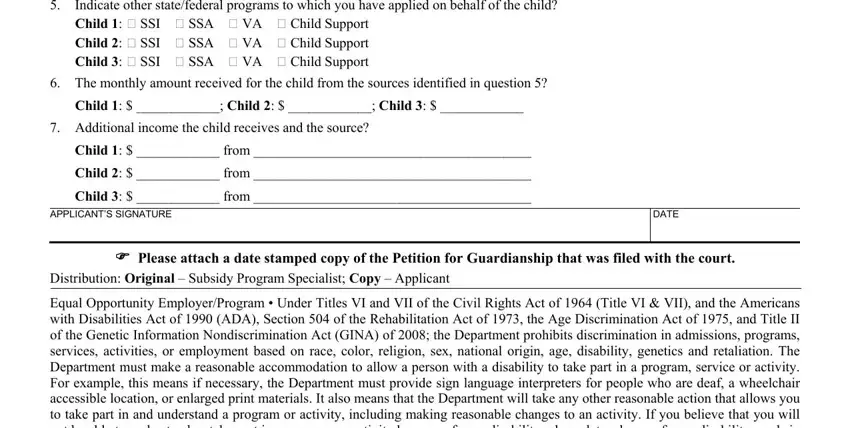
Fill out the Indicate other statefederal, The monthly amount received for, Child Child Child, Additional income the child, Child from, Child from, Child from, APPLICANTS SIGNATURE, DATE, Please attach a date stamped copy, Distribution Original Subsidy, and Equal Opportunity EmployerProgram areas with any information that may be requested by the software.
Step 3: Choose the "Done" button. Finally, you may export your PDF document - download it to your electronic device or send it by means of email.
Step 4: Ensure that you keep away from possible worries by creating no less than 2 copies of your file.
