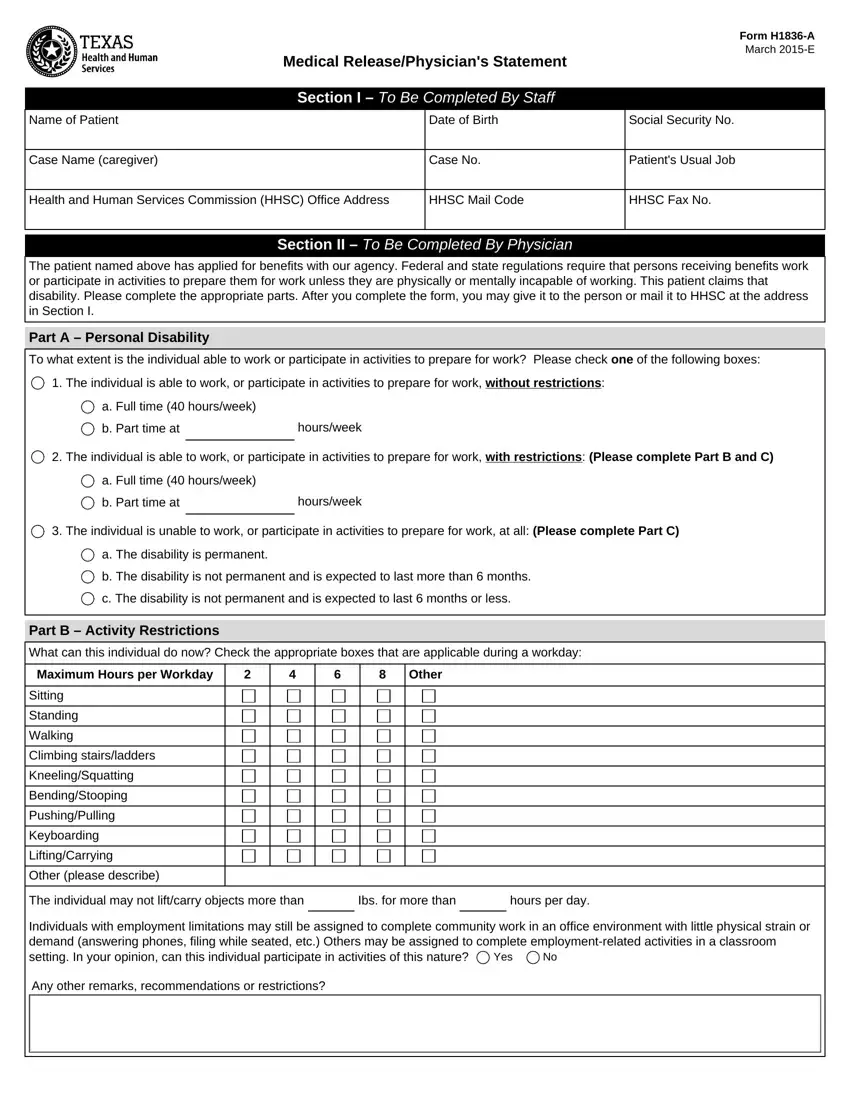
In the realm of healthcare and public assistance, navigating through the array of required forms and documentation can often seem daunting for both individuals and healthcare professionals alike. At the heart of this intricate process is the H1836-A form, a critical document designed to bridge the gap between medical assessments and eligibility for work-related exemptions in benefit programs. Officially titled the Medical Release/Physician's Statement, this form, as of its March 2015 iteration, mandates a thorough evaluation by a physician to ascertain an individual's capacity to engage in employment or employment-preparatory activities. The form is divided into distinct sections, each serving a unique purpose: the initial portion collects patient and case information through staff completion, while the subsequent sections delve into medical assessments exclusively completed by a physician. These assessments gauge the patient's ability to work, outline any restrictions, and provide a detailed account of the individual's diagnosis. Integral to this form is also the inclusion of a designated area for patient or their representative's authorization, allowing the release of pertinent medical information to the Health and Human Services Commission (HHSC) and the Texas Workforce Commission. This authorization facilitates the verification process of a medical condition that potentially hinders an individual's full participation in employment services programs, striking a fine balance between personal privacy and the need for informed evaluation in public assistance eligibility.
| Question | Answer |
|---|---|
| Form Name | H1836 A Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form 1836a, 1836 a, texas form 1836 a, hhsc form 1836a printable |
