With the purpose of making it as simple to use as it can be, we made the PDF editor. The process of filling up the how to hcfa 1500 is going to be quick when you consider the next steps.
Step 1: To get started, click the orange button "Get Form Now".
Step 2: You can find all of the options which you can use on your document after you have accessed the how to hcfa 1500 editing page.
Please enter the following information to complete the how to hcfa 1500 PDF:
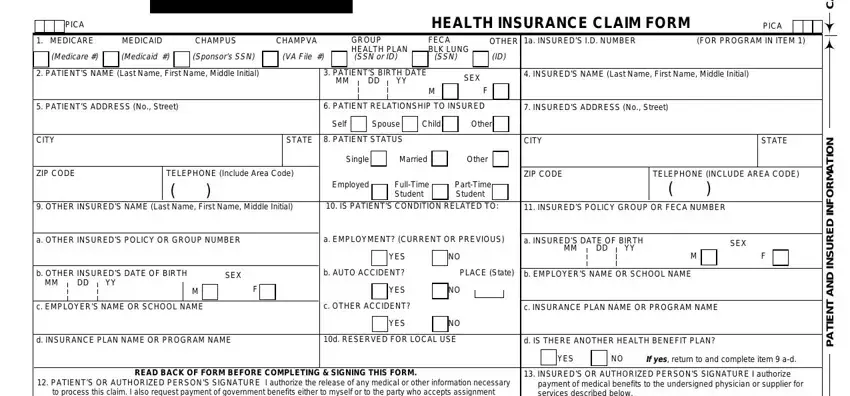
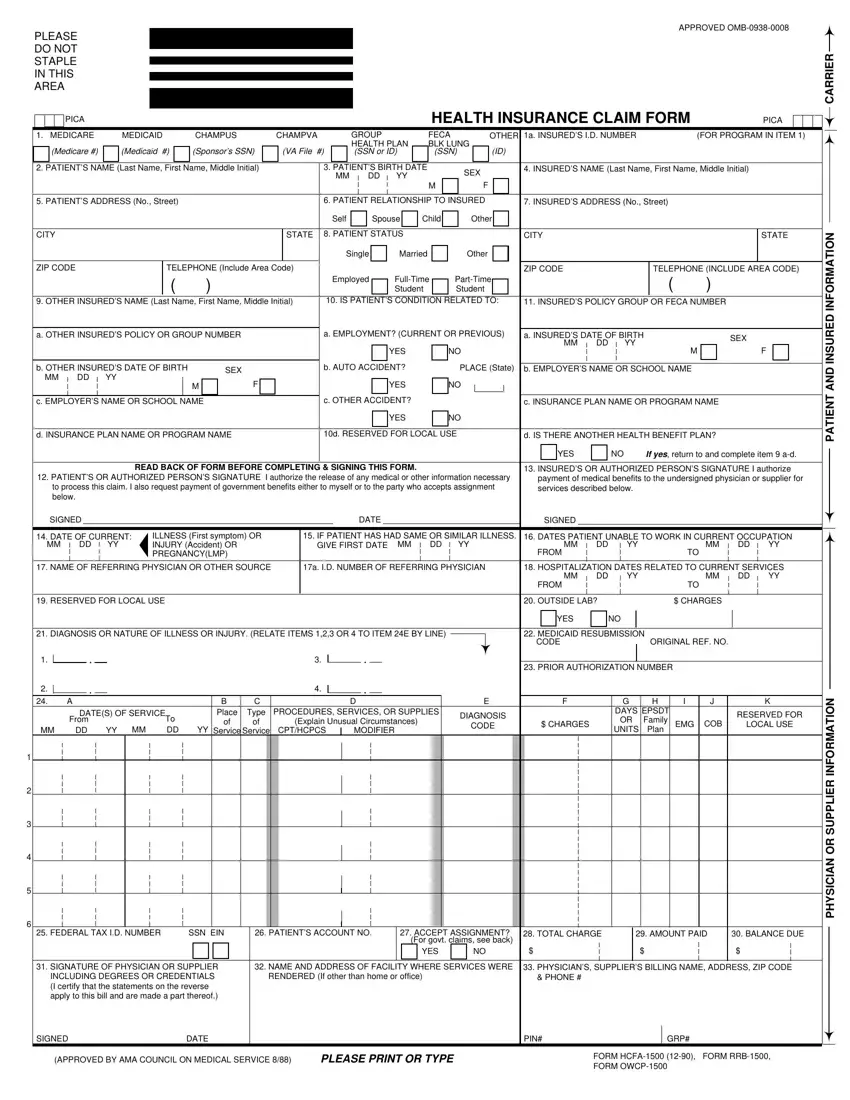
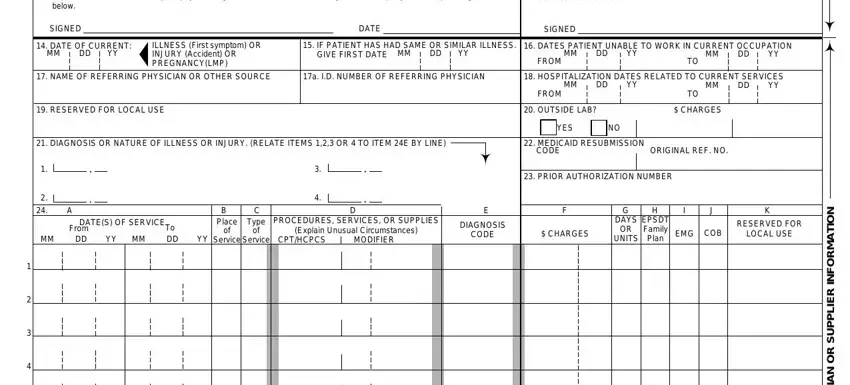
Provide the necessary data in the field READ BACK OF FORM BEFORE, payment of medical benefits to the, SIGNED, DATE OF CURRENT MM DD YY, ILLNESS First symptom OR INJURY, IF PATIENT HAS HAD SAME OR, GIVE FIRST DATE MM DD YY, FROM, DATES PATIENT UNABLE TO WORK IN, MM DD YY, MM DD YY, DATE, SIGNED, NAME OF REFERRING PHYSICIAN OR, and a ID NUMBER OF REFERRING PHYSICIAN.
Indicate the essential data in FEDERAL TAX ID NUMBER, SSN EIN PATIENTS ACCOUNT NO, ACCEPT ASSIGNMENT For govt claims, TOTAL CHARGE, AMOUNT PAID, BALANCE DUE, YES NO, SIGNATURE OF PHYSICIAN OR, NAME AND ADDRESS OF FACILITY, PHYSICIANS SUPPLIERS BILLING NAME, RENDERED If other than home or, PHONE, SIGNED, DATE, and PIN section.
Step 3: As soon as you select the Done button, your prepared file can be easily transferred to any of your gadgets or to email chosen by you.
Step 4: Make at least several copies of your form to stay away from any sort of potential future problems.
