The Health Assessment Sports Physical Statement (HASPS) for Child and Youth Services (CYS) enrollment and renewal details critical health information requirements and sports physical demands for participating in community activities, especially those related to sports. Crafted with the intent outlined by the Privacy Act of 1994, it aims to ensure children's safety by verifying health status, noting any special requirements or restrictions on participation due to health reasons, facilitating emergency medical procedures if necessary, and determining eligibility for the Exceptional Family Member Program. The form breaks down into three key parts: medical history provided by a parent or guardian, a physical examination by a licensed medical professional, and special medical considerations that might impact participation in CYS programs. The comprehensive nature of this form captures essential health metrics—from medical history, ongoing medications, allergies to detailed physical exam findings—while also addressing potential activity restrictions. It highlights the necessary immunization status and underscores the importance of assessing the child’s ability to partake in physical activities safely. Moreover, the form's structure underlines a collaborative approach between parents, guardians, and healthcare providers to ensure the well-being of the child, making it a crucial step for enrollment in sports and other CYS activities. Importantly, the voluntary disclosure of information dictates that without it, participation may be limited, emphasizing the critical role health plays in enabling active engagement in community and sport-related endeavors.
| Question | Answer |
|---|---|
| Form Name | Health Assessment Sports Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cys sports physical form, child and youth services health assessment sports physical, health assessment sports, cys health assessment form |
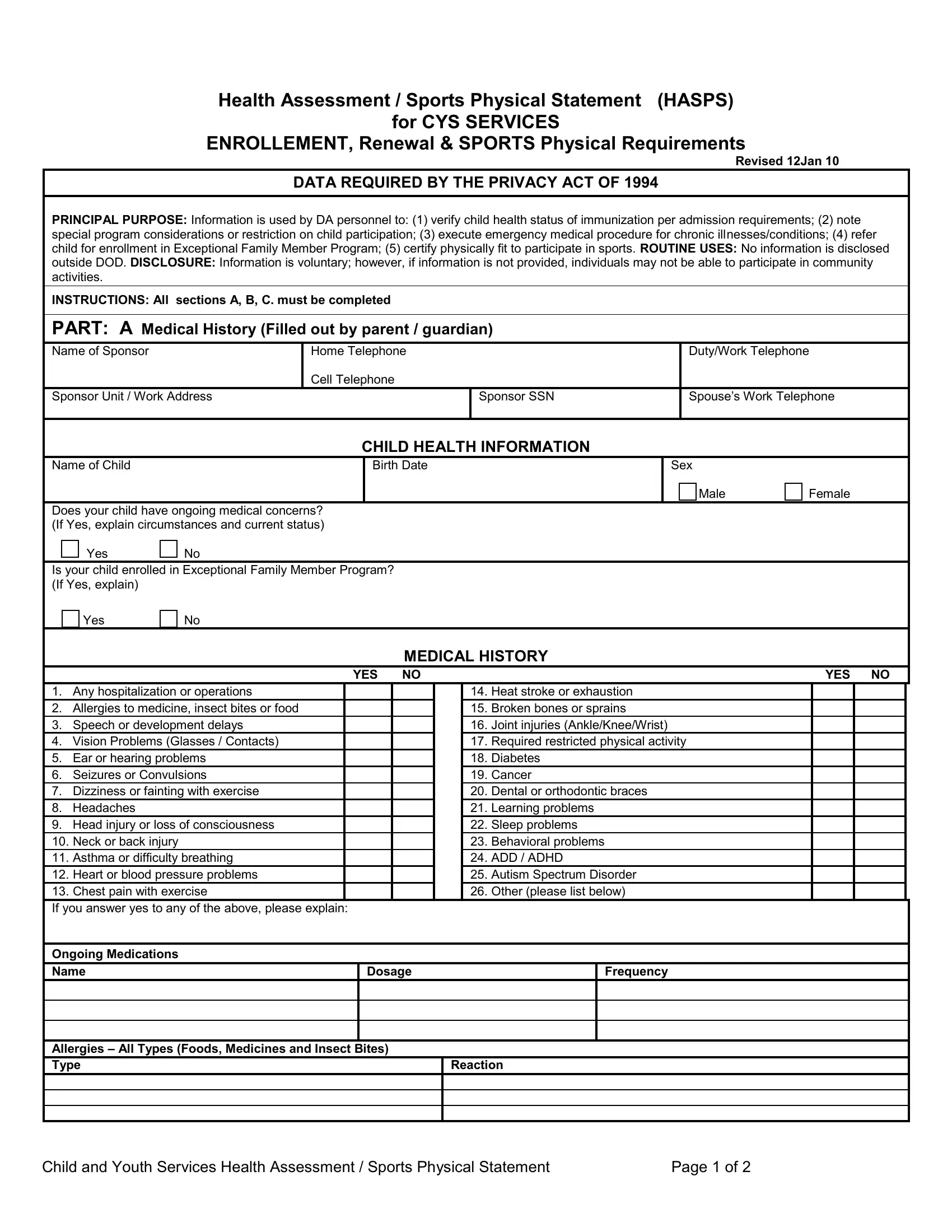
Health Assessment / Sports Physical Statement (HASPS)
for CYS SERVICES
ENROLLEMENT, Renewal & SPORTS Physical Requirements
Revised 12Jan 10
DATA REQUIRED BY THE PRIVACY ACT OF 1994
PRINCIPAL PURPOSE: Information is used by DA personnel to: (1) verify child health status of immunization per admission requirements; (2) note special program considerations or restriction on child participation; (3) execute emergency medical procedure for chronic illnesses/conditions; (4) refer child for enrollment in Exceptional Family Member Program; (5) certify physically fit to participate in sports. ROUTINE USES: No information is disclosed outside DOD. DISCLOSURE: Information is voluntary; however, if information is not provided, individuals may not be able to participate in community activities.
INSTRUCTIONS: All sections A, B, C. must be completed
PART: A Medical History (Filled out by parent / guardian)
|
Name of Sponsor |
Home Telephone |
|
Duty/Work Telephone |
|
|
|
Cell Telephone |
|
|
|
|
Sponsor Unit / Work Address |
|
Sponsor SSN |
Spouse’s Work Telephone |
|
|
|
|
|
|
|
CHILD HEALTH INFORMATION
Name of Child |
|
|
Birth Date |
Sex |
|
||
|
|
|
|
|
|
Male |
Female |
Does your child have ongoing medical concerns? |
|
|
|||||
(If Yes, explain circumstances and current status) |
|
|
|||||
|
|
Yes |
|
No |
|
|
|
Is your child enrolled in Exceptional Family Member Program? |
|
|
|||||
(If Yes, explain) |
|
|
|
|
|
||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
MEDICAL HISTORY |
|
|
YES NO
1.Any hospitalization or operations
2.Allergies to medicine, insect bites or food
3.Speech or development delays
4.Vision Problems (Glasses / Contacts)
5.Ear or hearing problems
6.Seizures or Convulsions
7.Dizziness or fainting with exercise
8.Headaches
9.Head injury or loss of consciousness
10.Neck or back injury
11.Asthma or difficulty breathing
12.Heart or blood pressure problems
13.Chest pain with exercise
If you answer yes to any of the above, please explain:
YES NO
14.Heat stroke or exhaustion
15.Broken bones or sprains
16.Joint injuries (Ankle/Knee/Wrist)
17.Required restricted physical activity
18.Diabetes
19.Cancer
20.Dental or orthodontic braces
21.Learning problems
22.Sleep problems
23.Behavioral problems
24.ADD / ADHD
25.Autism Spectrum Disorder
26.Other (please list below)
Ongoing Medications
Name |
Dosage |
Frequency |
|
|
|
|
|
|
|
|
|
Allergies – All Types (Foods, Medicines and Insect Bites)
Type |
Reaction |
|
|
|
|
|
|
Child and Youth Services Health Assessment / Sports Physical Statement |
Page 1 of 2 |
PART B: Physical Exam
Medical Staff Assessment (Completed by licensed independent practitioner:
Age |
|
Height |
|
|
|
Weight |
|
YRS |
MOS |
__________ cm. |
( _____ %ile) |
|
__________ kgs. |
(_____ %ile) |
|
BP: |
/ |
Visual Acuity |
|
|
|
|
|
P: |
|
Right |
/ |
Left |
/ |
Tested with / without glasses |
|
|
|
|
|
|
|
||
|
|
NORMAL |
ABNORMAL N / A |
COMMENTS |
|
||
1.Eyes
2.Ears, Nose & Throat
3.Hearing
4.Mouth & Teeth
5.Neck (Soft tissues)
6.Cardiovascular
7.Chest & Lungs
8.Abdomen
9.Genitalia – Hernia
10.Skin & Lymphatics
11.Spine – Scoliosis
12.Extremities
13.Neurological
14.Wears braces / plates
Based on this HX and PX exam, the following abnormalities were found and may need treatment:
Immunizations are current and up to date: |
|
Yes |
|
No |
|
|
PARTICIPATION RECOMMENDATIONS
All sports |
_____Yes _____ No |
Additional comments:
Normal physical activity to including PE
Restrictions:
Sports Physical is valid for 1 year from date indicated below
PART C
Special Medical Considerations: Describe any special program needs, considerations or restrictions which the child requires in order to participate in CYS programs (to include Sports).
Child / Youth is able to participate in normal CYS programs?
Yes
No
Date |
Licensed Health Care Professional Stamp |
Licensed Health Care Professional; Dr., NP or PA Signature |
Initial DateType or print name of Parent or GuardianSignature of Parent or Guardian
HASPS Renewal (Not Part of the Sports Physical)
Year 2 Date |
Health Status Changed |
Signature of Parent or Guardian |
|
|
Yes |
No |
|
|
|
|
|
Year 3 Date |
Health Status Changed |
Signature of Parent or Guardian |
|
|
Yes |
No |
|
Child and Youth Services Health Assessment / Sports Physical Statement |
Page 2 of 2 |