
Emdeon can be filled out online effortlessly. Just open FormsPal PDF tool to finish the job right away. To maintain our editor on the leading edge of efficiency, we work to put into operation user-driven capabilities and enhancements on a regular basis. We are routinely looking for suggestions - join us in revampimg the way you work with PDF files. Here is what you would have to do to get started:
Step 1: First, access the pdf tool by pressing the "Get Form Button" at the top of this site.
Step 2: This editor enables you to change PDF forms in a variety of ways. Transform it by writing your own text, correct existing content, and include a signature - all within a couple of mouse clicks!
As for the fields of this precise PDF, this is what you should do:
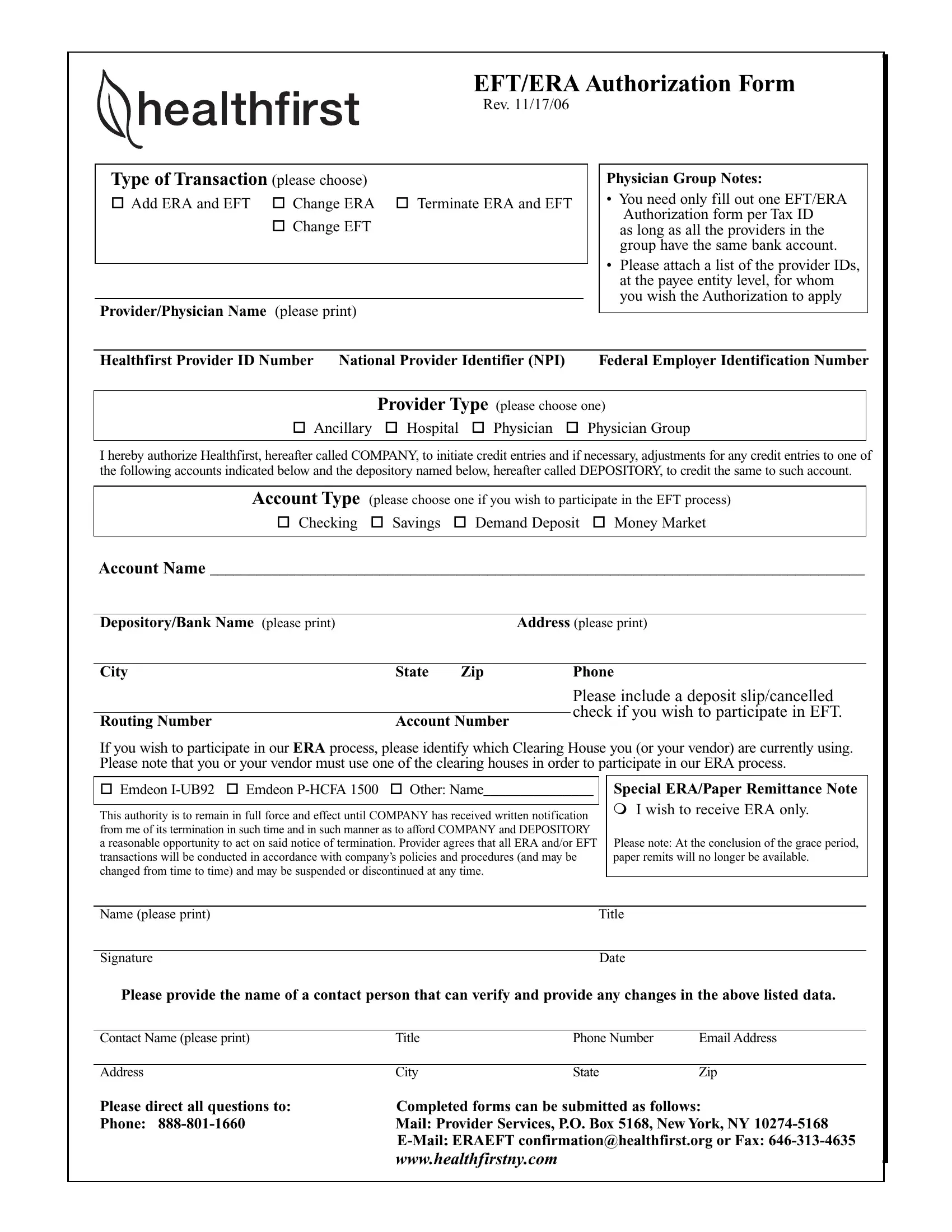
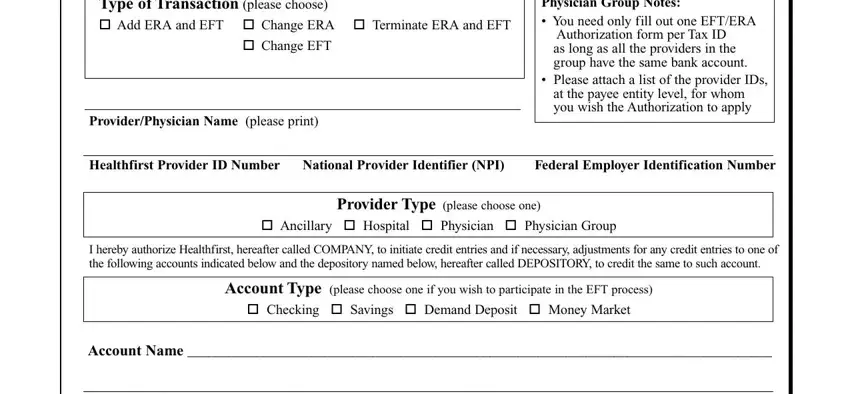
1. Start filling out your Emdeon with a number of major blanks. Gather all of the required information and make sure nothing is left out!
2. Once your current task is complete, take the next step – fill out all of these fields - DepositoryBank Name please print, Address please print, City, State, Zip, Phone, Routing Number, Account Number, Please include a deposit, If you wish to participate in our, Emdeon IUB Emdeon PHCFA Other, Special ERAPaper Remittance Note m, This authority is to remain in, Name please print, and Signature with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
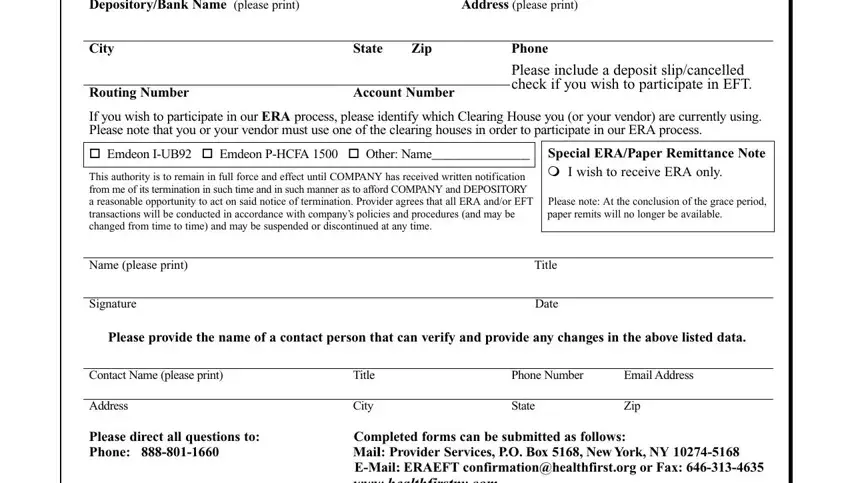
It is easy to get it wrong when filling out the City, for that reason make sure that you take another look before you decide to submit it.
Step 3: Go through all the information you have inserted in the form fields and then click the "Done" button. Obtain your Emdeon once you join for a 7-day free trial. Conveniently use the pdf in your FormsPal cabinet, along with any edits and changes conveniently synced! Here at FormsPal.com, we endeavor to ensure that your details are stored secure.