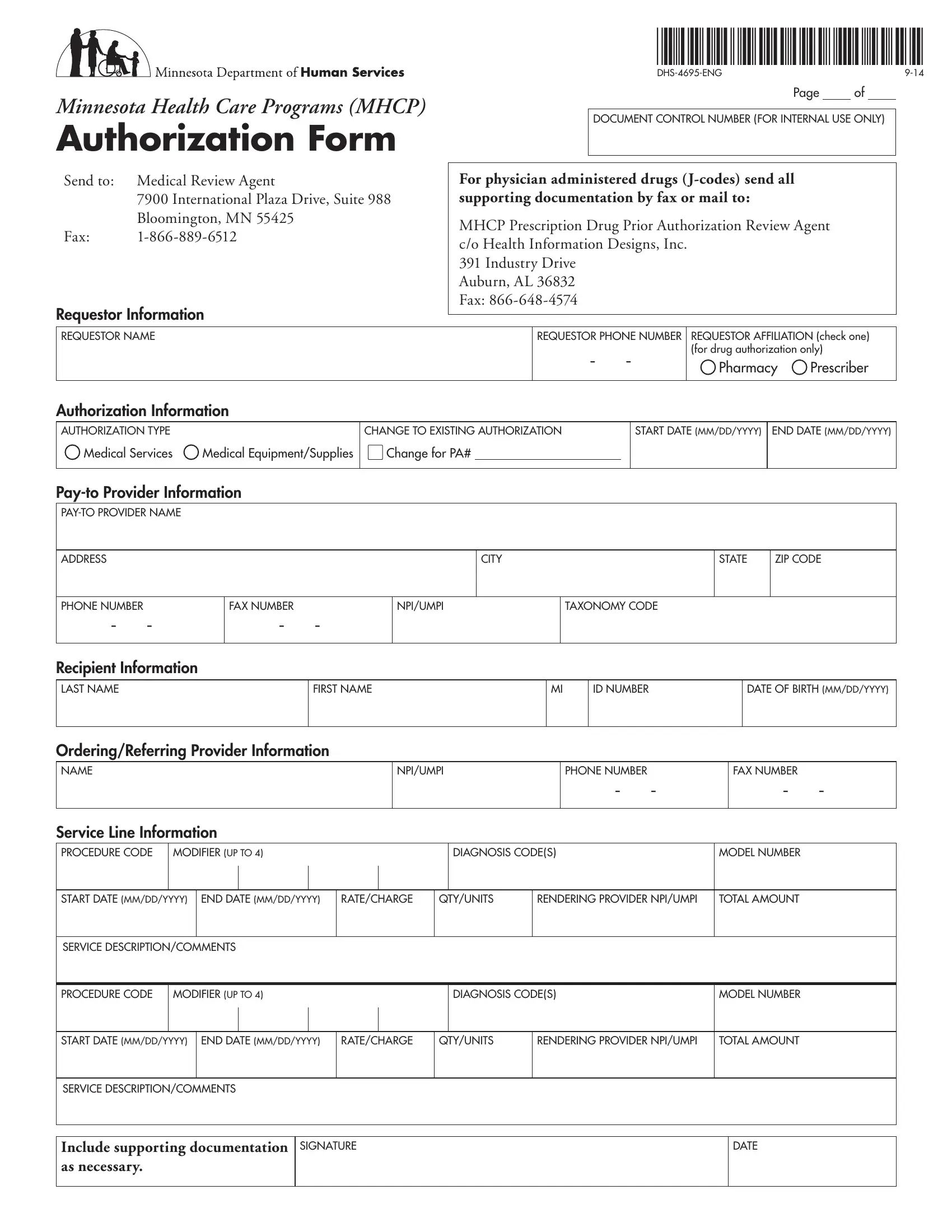
The Minnesota Health Care Programs (MHCP) Authorization Form, identified by its form number DHS-4695-ENG, serves as a critical document in the administration of medical services, medical equipment, and supplies involving MHCP enrollees. This comprehensive form is designed to streamline the process of seeking authorization for a wide range of medical services and products by healthcare providers. It encompasses various sections including requestor information, authorization data, provider and recipient details, as well as service line information. Providers are prompted to fill in details ranging from the nature of the authorization request, pertinent dates for the start and end of the service, through to specific codes for procedures, diagnosis, and equipment. Additionally, the form mandates the inclusion of the provider’s information such as National Provider Identifier (NPI) or Universal Medical Provider Identification (UMPI), contact details, and information regarding the pay-to provider. This form not only demands precise information regarding the medical service or equipment requested but also underscores the need for supporting documentation to ensure a comprehensive review. Fulfillment of the form’s requirements facilitates the review process by Medical Review Agents and aids in the timely provision of essential healthcare services to recipients.
| Question | Answer |
|---|---|
| Form Name | Mhcp Authorization Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | mhcp authorization, mhcp form, dhs 4695 eng, dhs4695 eng form |