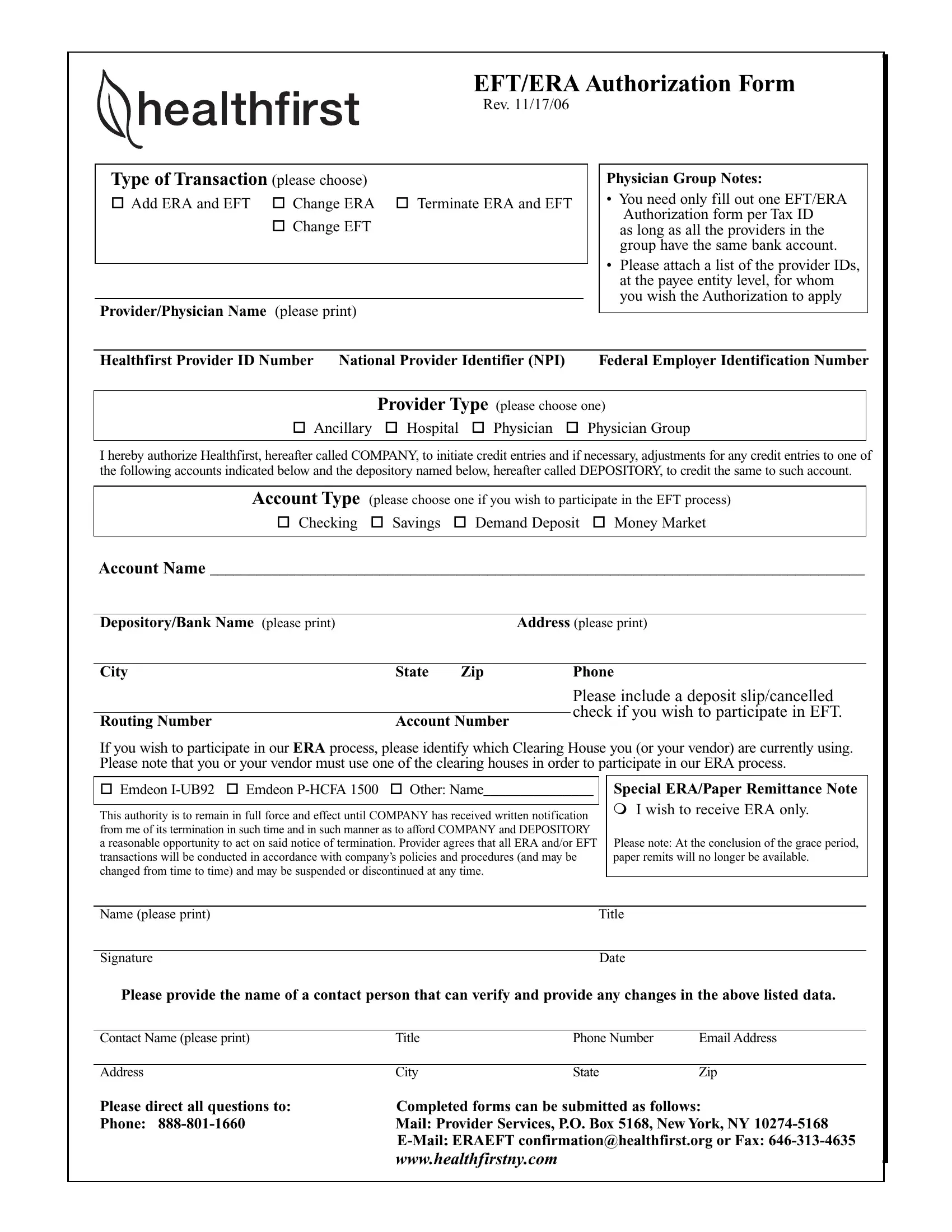
The Healthfirst Electronic Funds Transfer (EFT) and Electronic Remittance Advice (ERA) Authorization form is a crucial document for healthcare providers who wish to streamline their financial transactions with Healthfirst. Revised on November 17, 2006, this form allows for several types of transactions, including the addition or change of ERA and EFT settings, and the termination of these services. To ensure a smooth and unified process, it's required that only one form is filled out per tax ID, given that all providers within a group utilize the same banking account. Along with this form, it's necessary to attach a list of provider IDs to signify whose authorizations are being requested. Providers can choose between bank account types for EFT such as checking, savings, demand deposit, or money market accounts. Additionally, for ERA participation, the form inquires about the clearinghouse used by the provider or their vendor, emphasizing the necessity to use one of the listed clearinghouses to avail of ERA services. This authorization remains active until Healthfirst receives a written termination notice providing sufficient time for proper processing. It's highlighted that any ERA and EFT transactions will abide by Healthfirst's policies, which may be subject to change, and can be discontinued anytime. Providers preferring only ERA services must note this specifically, keeping in mind that paper remittances become unavailable after a grace period. The form also requests contact information for follow-ups and directs where to submit completed forms, providing multiple submission options including mail, email, and fax, ensuring accessible support for providers.
| Question | Answer |
|---|---|
| Form Name | Healthfirst Eft Era Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Emdeon, healthfirst eft authorization form, healthfirst eft era authorization form, remits |