Are you a member looking to gain access to certain services or resources? If so, you may need to submit an authorization form. Authorization forms are often required when requesting particular private information, new accounts with financial institutions, and other membership applications. In this blog post, we will explore the basics of a member authorization form and why it is important. We'll also provide all the key details that should go into one before submission.
| Question | Answer |
|---|---|
| Form Name | Member Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cvs caremark prior auth form, cvs caremark prior authorization form pdf, Rx, Caremark |
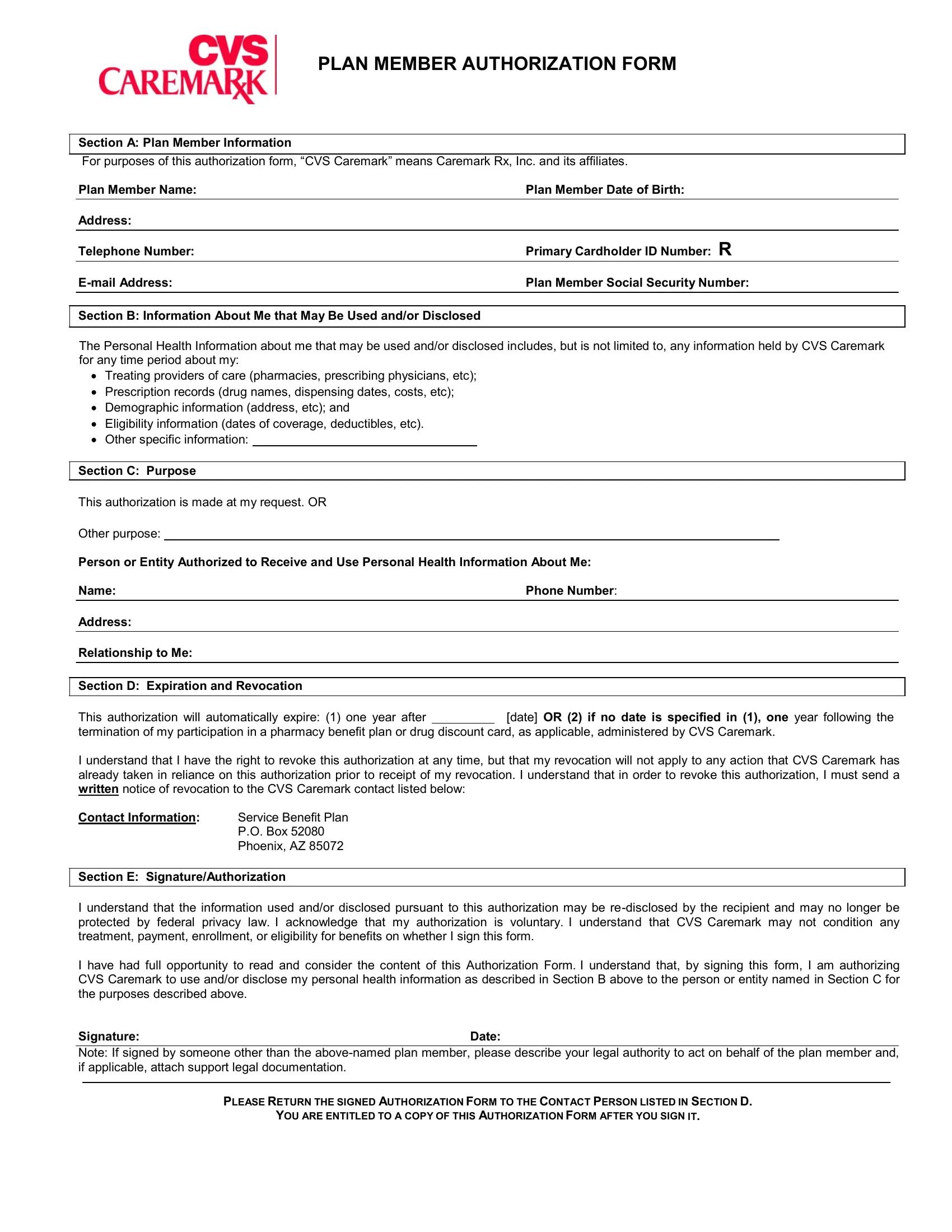
PLAN MEMBER AUTHORIZATION FORM
Section A: Plan Member Information
For purposes of this authorization form, “CVS Caremark” means Caremark Rx, Inc. and its affiliates.
|
Plan Member Name: |
Plan Member Date of Birth: |
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
Telephone Number: |
Primary Cardholder ID Number: R |
|
|
Plan Member Social Security Number: |
|
|
|
|
|
|
|
|
|
|
|
Section B: Information About Me that May Be Used and/or Disclosed |
|
|
|
|
|
|
The Personal Health Information about me that may be used and/or disclosed includes, but is not limited to, any information held by CVS Caremark for any time period about my:
∙Treating providers of care (pharmacies, prescribing physicians, etc);
∙Prescription records (drug names, dispensing dates, costs, etc);
∙Demographic information (address, etc); and
∙Eligibility information (dates of coverage, deductibles, etc).
∙Other specific information:
Section C: Purpose
This authorization is made at my request. OR
Other purpose:
Person or Entity Authorized to Receive and Use Personal Health Information About Me:
Name: |
Phone Number: |
|
|
Address:
Relationship to Me:
Section D: Expiration and Revocation
This authorization will automatically expire: (1) one year after [date] OR (2) if no date is specified in (1), one year following the
termination of my participation in a pharmacy benefit plan or drug discount card, as applicable, administered by CVS Caremark.
I understand that I have the right to revoke this authorization at any time, but that my revocation will not apply to any action that CVS Caremark has already taken in reliance on this authorization prior to receipt of my revocation. I understand that in order to revoke this authorization, I must send a written notice of revocation to the CVS Caremark contact listed below:
Contact Information: |
Service Benefit Plan |
|
P.O. Box 52080 |
|
Phoenix, AZ 85072 |
Section E: Signature/Authorization
I understand that the information used and/or disclosed pursuant to this authorization may be
I have had full opportunity to read and consider the content of this Authorization Form. I understand that, by signing this form, I am authorizing CVS Caremark to use and/or disclose my personal health information as described in Section B above to the person or entity named in Section C for the purposes described above.
Signature:Date:
Note: If signed by someone other than the
PLEASE RETURN THE SIGNED AUTHORIZATION FORM TO THE CONTACT PERSON LISTED IN SECTION D.
YOU ARE ENTITLED TO A COPY OF THIS AUTHORIZATION FORM AFTER YOU SIGN IT.